Playlist
Show Playlist
Hide Playlist
Large Intestines: Colon Volvulus


-
Slides Volvulus General Surgery.pdf
-
Download Lecture Overview
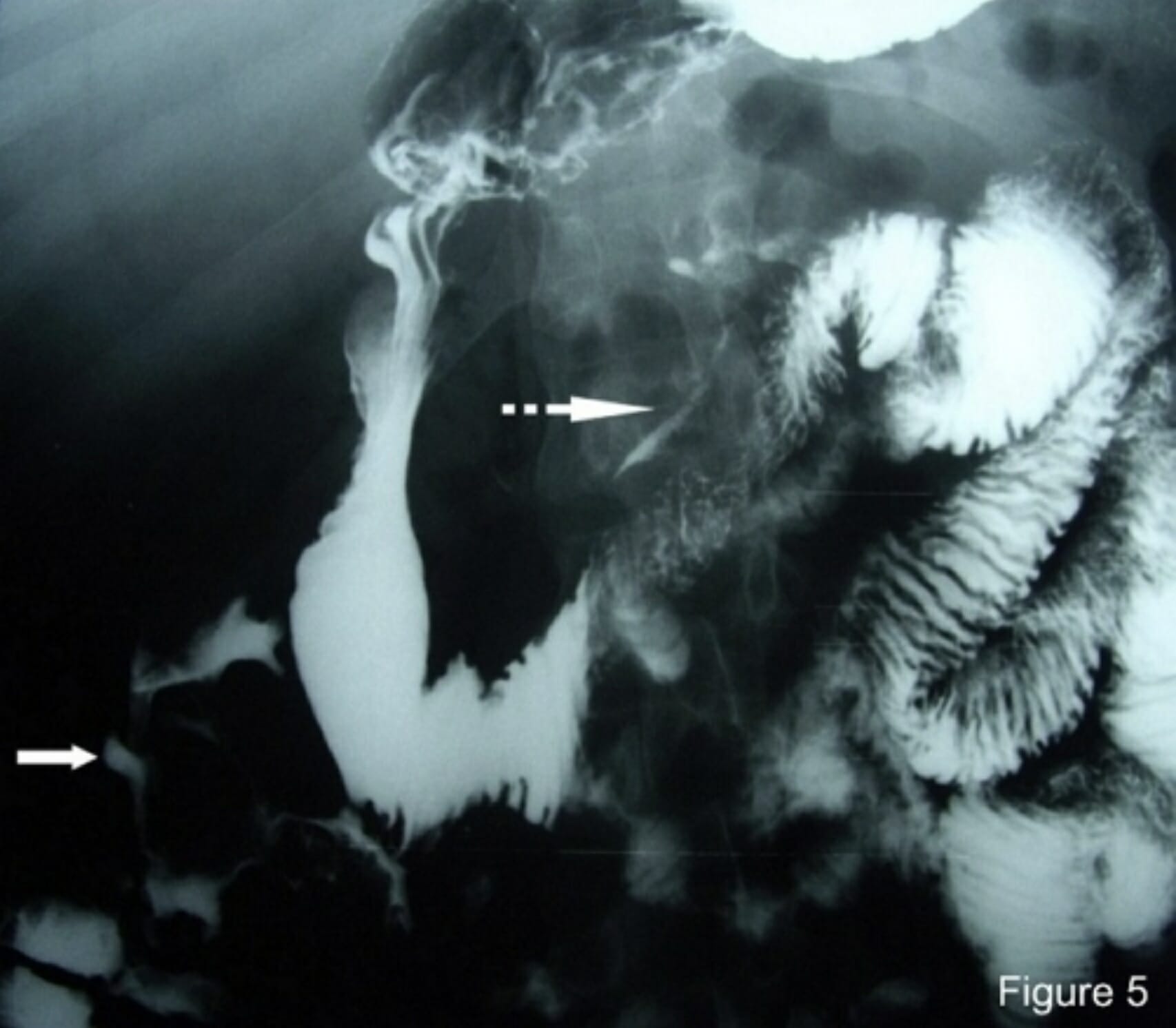
00:01 Welcome back. Thanks for joining me on this discussion of colon volvulus in this section of large intestines. Take a look at this intraoperative picture. You see that big distended loop of bowel that’s in the center of the picture? That’s likely the result of volvulus or twisting of the large intestines. It particularly starts contrasting next to the normal sized small intestines in the middle of the screen. What are the causes of volvulus? We typically think of two things that have to happen. You have to have a redundant colon and portions of that are not attached. 00:39 This allows for twisting of the intestines particularly the large intestines. In the redundancy of the colon, the sigmoid colon is particularly a classic representation of volvulus. The sigmoid colon by nature is anatomically floppy and mobile. What about unattached colons? Portions of the colon normally are attached to the abdominal wall. Recall during your surgical clerkships where you saw intraoperatively that the colons were attached to the lateral walls by a structure called the white line of Toldt,T-O-L-D-T. In certain patients, whether it’s the cecum or the sigmoid colon, these anatomic regions of the attachment are not present or only partially present. 01:26 Therefore, the combination of redundant colon and unattached portions of the colon is a setup for volvulus. As I mentioned, volvulus occur at points of potential colon redundancy and areas of lack of attachment. This again can either be the cecum or the sigmoid colon, although very much more commonly in the sigmoid colon; the majority in the sigmoid colon followed by the cecum. 01:54 Take a look at this intraoperative picture. It’s different than the first picture we looked at mainly because as you can see, segments of the colon are ischemic. Contrast the right side of the screen to the left side of the screen where you see left side of the screen is distended and dilated colon but it appears viable as opposed to the right side of the screen where the colon is clearly ischemic and dead. This patient had what’s called the cecal bascule which is another word for volvulus, likely, waited too long for surgery and therefore became ischemic. Take another look at this picture. This is a sigmoid volvulus. Look at the very distended loop of intestines that’s twisted on itself. This is large intestines. What are some physical findings of volvulus? Well, depending on which segment of the colon is volvulized, you may have what I said a right quadrant abdominal pain when it’s involving cecal volvulus. You may have left side lower abdominal pain when it's involving the sigmoid. Remember that the sigmoid colon tends to be floppy. Particularly in a very distended abdomen, it may be very difficult for you to localize. Oftentimes, patient will have significant amount of abdominal distension, not necessarily associated, the distension itself is not necessarily associated with the level or severity of pain. What laboratory workup is indicative of volvulus? Well, not a whole lot. Your chemistries may be normal. You may have an increased white blood cell count. I like to just remind you again that anytime a patient has small intestines or large intestines obstruction volvulus, when those patients demonstrate an increased white blood cell count or leukocytosis, one should have a lower threshold for going to the operating room. There are some characteristic abdominal X-ray findings suggestive of a sigmoid or cecal volvulus. But I would like to caution you that classic findings are rare. Notice these images with the direction of the arrow. 04:05 So, if you think of an inner bent tube, inner tube and you have a tube at sigmoid of colon that’s wrapped in upside down u-shape, the apex of that u is the direction of the arrows. 04:17 The direction of the arrow is suggestive. If the apex points to the right upper quadrant that it's a sigmoid volvulus as opposed to an inner tube that has the apex pointing over to the left upper quadrant of the abdomen suggestive of potentially a cecal volvulus. Here, we recommend colonic decompression for sigmoid volvulus. You’ll notice that this patient’s abdomen is quite distended. 04:49 Oftentimes, the first thing to do to try to prevent perforation or further distension of the abdomen is to perform a colonoscopic decompression. Also notice that the colonic decompression is not only to get rid of the air but also one can untwist the sigmoid volvulus. When is surgery indicated? Generally, all patients except the most critically ill should undergo surgery. Why is that? Because patients with volvulus, whether it’s cecal or sigmoid are likely to recur without surgery. 05:22 Laparoscopic or open sigmoid colectomy for sigmoid volvulus or laparoscopic or open right hemicolectomy for a cecal volvulus, these are considered definitive operations. Now remember, during these partial resections of segments of colon, there is no rule to say you can’t put the colon back together or what’s called a primary anastomosis. However, in the setting of extreme dilation due to the volvulus, oftentimes it’s necessary to do a temporizing or permanent ostomy. 05:55 This slide demonstrates to you a segmental sigmoid resection with either a colostomy or a colopexy. 06:04 Now, recall that I said that most patients except the most critically ill should undergo surgery. 06:10 Colopexy is not the most ideal surgery. Colopexy means pexy or tacking portions of the colon to the abdominal wall. Recall that one of the things that sets you up for a sigmoid volvulus is a lack of attachment. We do not consider that definitive therapy. So, if one undertakes surgery, it’s better to complete the sigmoid resection with or without primary anastomosis. Here is a picture of a cecal volvulus. Patients can undergo recall a laparoscopic, in this situation, in this image demonstrates laparoscopic trocar placements with an extracorporeal or outside of the abdominal wall anastomosis or connection. This, of course, can be done as an open procedure but this is the definitive therapy for cecal volvulus. Sometimes there are also patients who undergo a cecostomy which is a temporary blowhole, if you will. We do not again consider that definitive therapy, unless it’s for the most critically ill patients. How do we prevent volvulus? We avoid constipation and have regular bowel movements. Aside from that, there is not much you can do. Why? Because there’s an anatomic reason why the patient developed volvulus. Some important clinical pearls: If the patient develops cecal volvulus, it’s usually ill-advised to do a colonoscopic decompression because as you remember, governed by the LaPlace's Law, the cecum is most likely to perforate. 07:40 The cecum is most likely to perforate because it’s also the thinnest wall. The likelihood of perforation and the tension on the wall is proportional to the radius. For your examination, please remember when surgery is performed in an emergent setting, you may need to place an ostomy after resection of the sigmoid colon. If the patient can safely undergo surgery, it is best to perform the definitive therapy whether it’s a right hemicolectomy or a left hemicolectomy depending on the side of the volvulus. 08:17 Thank you very much for joining me on this discussion of colonic volvulus.
About the Lecture
The lecture Large Intestines: Colon Volvulus by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which of the following statements about colonic volvuli are FALSE?
- The white line of Toldt attaches the ascending and descending colon medially which helps to prevent colonic volvulus.
- Volvulus may involve the sigmoid colon.
- A redundant colon increases the risk of volvulus.
- A non-attached colon increases the risk of volvulus.
- Volvulus may sometimes involve the cecum.
Which part of the colon is most commonly involved in volvulus?
- Sigmoid
- Cecum
- Ascending colon
- Descending colon
- Transverse colon
Which of the following presentations is NOT matched correctly with its cause?
- X-ray with bent inner tube sign where the apex of the U shape points towards the groin --- sigmoid volvulus
- Right quadrant abdominal pain --- cecal volvulus
- Left quadrant abdominal pain --- sigmoid volvulus
- Abdominal distention --- cecal volvulus
- Diffuse abdominal pain --- sigmoid volvulus
Which of the following statements is TRUE about the management of volvulus?
- Sigmoid colectomy is the definitive treatment for sigmoid volvulus.
- Colonoscopic decompression is the first step in treating cecal volvulus.
- Colopexy is a definitive surgical repair of volvulus.
- Cecal decompression with a colostomy is a definitive treatment of cecal volvulus.
- Colonoscopic decompression is the definitive treatment for sigmoid volvulus.
According to Laplace’s law, which area of the colon is most likely to perforate if involved in a volvulus?
- Cecum
- Sigmoid
- Ascending colon
- Descending colon
- Transverse colon
Author of lecture Large Intestines: Colon Volvulus

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
