Playlist
Show Playlist
Hide Playlist
Lambert Eaton Myasthenic Syndrome (LEMS): Workup and Testing

-
Slides Strowd Neoplastic or Paraneoplastic NMJ Disorders.pdf
-
Download Lecture Overview
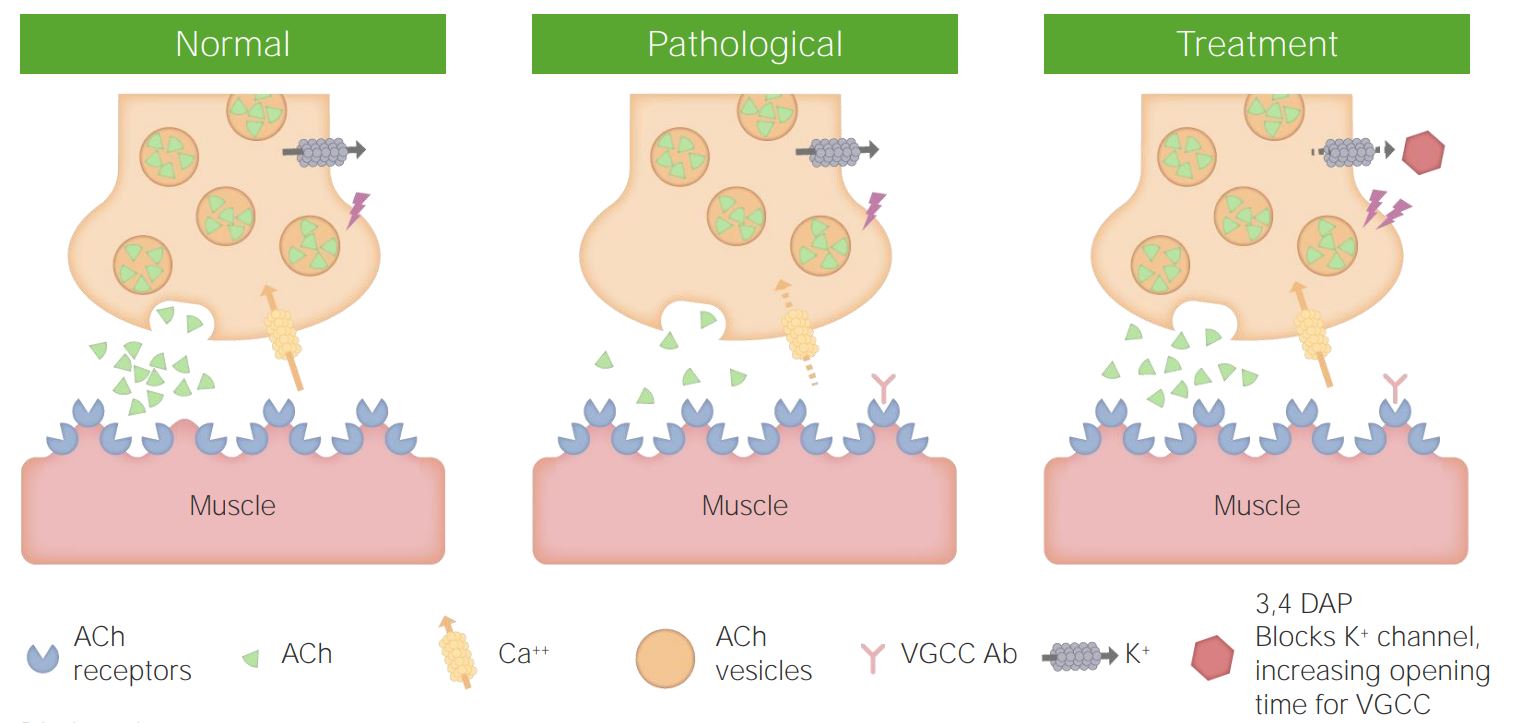
00:01 So what's the typical work up for a patient, who were concerned may have Lambert-Eaton myasthenic syndrome? Well, we've talked about nerve conduction studies and that's critical of for evaluating the neuromuscular junction. 00:12 For looking at the nerve, at the muscle and how they're communicating. 00:17 The nerve conduction study for Lambert-Eaton myasthenic syndrome may show neuropathic findings. 00:23 And this is a typical because it's not a nerve condition, but we can see those findings. 00:28 We look for three things in the nerve conduction study for a patient with Lambert-Eaton syndrome. 00:34 The first is Reduced CMAP Amplitude- compound muscle action potential, reduced action of the muscle. 00:42 We can see a decremental response with low frequency stimulation 3-Hz stimulation. 00:47 And this is indicative of a neuromuscular junction disorder. 00:50 We see the same decremental response or can see this response with any neuromuscular junction condition. 00:57 And then importantly the 3rd point here is really important. 01:01 We see an incremental response with high-frequency stimulation. 01:04 This is unique to Lambert-Eaton syndrome and it is diagnostic of a presynaptic junctional disorder. 01:11 An incremental response with high frequency repetitive nerve stimulation. 01:17 This is an immune mediated condition, so we look for those immune cells and lab testing should include. 01:23 Tests for voltage-gated calcium channel antibodies in the serum. 01:27 And this is commonly seen in these patients. 01:29 And then it's associated with cancer, so we need to screen for cancer. 01:33 And we do prod widespread cancer screening, but particularly look for lung cancers or possible lymphomas, which are most associated with this condition. 01:43 Let's focus more on the nerve conduction testing for Lambert-Eaton syndrome. 01:48 Repetitive nerve stimulation is key to evaluating a neuromuscular junction disorder, and we're looking for two findings that are both sensitive and specific for a diagnosis of Lambert-Eaton syndrome. 02:00 The first is we see a decrement in the CMAP amplitude- the compound motor action potential, a decrement in the response of greater than 10% with low frequency stimulation. 02:11 With 3-Hz stimulation, we see that decrement in the signal that transfers from the nerve to the muscle and the contraction of the muscle. 02:19 Importantly the second finding that is diagnostic of lambert-eaton syndrome or a presynaptic terminals problem is an incremental response with fast or fast hertz repetitive stimulation. 02:30 So we see an increment in the CMAP amplitude of greater than a hundred percent at high-frequency stimulation or with post exercise testing. 02:40 This incremental response is due to increased release of calcium as a result of repeated stimulation. 02:46 We're overriding those calcium channels, we're driving acetylcholine into the presynaptic terminus and release into the synaptic cleft and allowing that muscle to contract even more than it did, at baseline. 02:58 In terms of serologic testing we test for the voltage-gated calcium channel antibodies. 03:03 Those are PQ type voltage-gated calcium channel antibodies and testing should be performed in all patients suspected of Lambert-Eaton syndrome. 03:11 We see these antibodies in about 85 to 90% of patients who have limbs. 03:16 So the presence of a voltage gated calcium channel antibody in someone who has weakness and a concern for cancer is diagnostic of Lambert-Eaton syndrome. 03:26 Cancer screening is also important, and here's the chest CT for the patient from our case. 03:31 We do both chest x-rays and chest CT's to look for findings of a lung cancer and particularly a small cell lung cancer and may also need to do screening for Lymphoma or other cancers, if our initial workup for cancer is negative. 03:44 And here you can see a large lesion in the right lobe of the lung highlighted by this green arrow that in this patient with rapid weight loss is consistent or concerning for a diagnosis of cancer and would be biopsied for further evaluation
About the Lecture
The lecture Lambert Eaton Myasthenic Syndrome (LEMS): Workup and Testing by Roy Strowd, MD is from the course Disorders of the Neuromuscular Junctions.
Included Quiz Questions
Which of the following is not associated with Lambert-Eaton myasthenic syndrome?
- Incremental response with low-frequency repetitive stimulation
- Presence of small cell lung cancer
- Calcium channel antibodies in the serum
- Reduced compound muscle action potential amplitude
- Incremental response with high-frequency stimulation
Which of the following is not involved in the diagnosis of Lambert-Eaton myasthenic syndrome?
- Improvement with AChE inhibitor administration
- The decrement of compound motor action potential amplitude of >10% at low-frequency stimulation
- Increments of compound motor action potential amplitude of >100% with high-frequency stimulation
- Presence of voltage-gated calcium channel antibodies in someone with weakness and concern for cancer
- Increments of compound motor action potential amplitude of >100% at with post-exercise testing
Author of lecture Lambert Eaton Myasthenic Syndrome (LEMS): Workup and Testing

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
