Playlist
Show Playlist
Hide Playlist
Lambert Eaton Myasthenic Syndrome (LEMS): Overview

-
Slides Strowd Neoplastic or Paraneoplastic NMJ Disorders.pdf
-
Download Lecture Overview
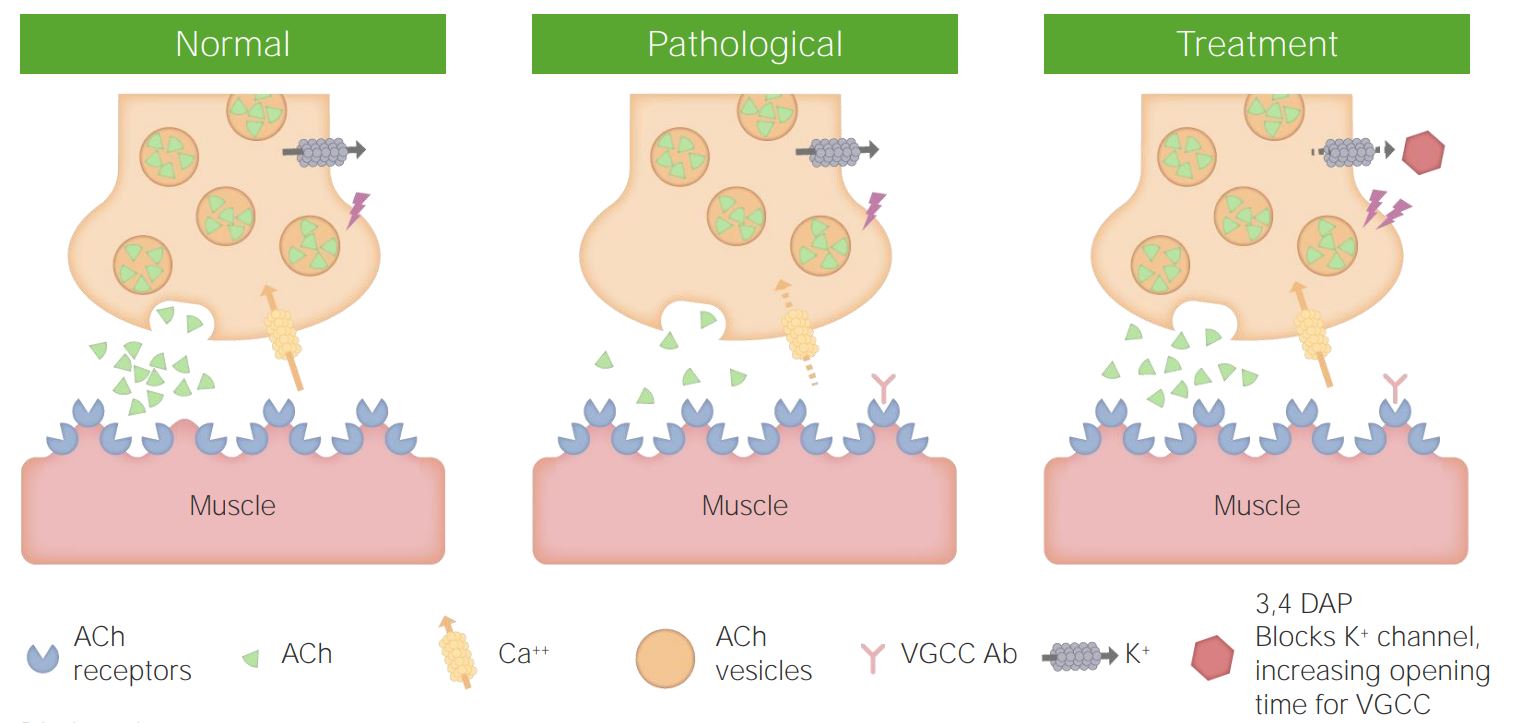
00:01 So let's learn a little bit more about Lambert-Eaton Myasthenic Syndrome. 00:05 What is it? And how does it work? Well, first of all, it's a rare disease. 00:09 Some neurologists go their whole career without seeing this, but we're always tested on it. 00:14 It's one of those conditions that test questions like, that board exams love to test about and you really need to know in order to recognize it. 00:23 It is an autoimmune disorder, and frequently it is a paraneoplastic immune disorder And that means the immune system is revved up to fight a cancer like a new lung cancer perhaps in our patient. 00:35 And as a result of revving up the immune system to fight the cancer something happens and the immune system goes awry and starts to attack a certain part of the body. 00:45 For Lambert-Eaton myasthenic syndrome, we see the development of autoreactive antibodies to the presynaptic voltage-gated calcium channel. 00:53 Those important calcium channels that recognize the action potential in the nerve that bring calcium in to the pre-synaptic terminus and drive the release of acetylcholine into the neuromuscular junction, so that muscles can move. 01:07 This condition is associated with certain types of cancer. 01:10 And we think of and most commonly we see, small cell lung cancers and lymphomas. 01:16 Other cancers have been described but those are the two things to think about, and focus on and evaluate for a patient who may have Lambert-Eaton myasthenic syndrome. 01:26 How the patients present? Well, proximal weakness is common as we see with many neuromuscular junction disorders. 01:33 It is often proximal and then spreads distally. 01:36 And importantly, this is a neuromuscular junction disorder and we see bulbar symptoms. 01:41 That's that critical distribution that points towards a problem in the neuromuscular junction. 01:47 So we look for ptosis, diplopia, dysarthria, dysphagia. 01:50 And here we see in the image a patient with right-sided ptosis. 01:54 Something to focus on and look for on our neurological exam. 01:58 There's a paucity of century findings, we usually don't hear about numbness or tingling or paresthesias. 02:04 Areflexia can be seen or hyporeflexia. 02:08 And this is important. 02:10 We said with neuromuscular junction disorders, we typically see normal to reduced reflexes. 02:16 And this is the one neuromuscular junction condition that can actually present with areflexia. 02:21 So an important caveat, an exception to our neuromuscular junction rule. 02:26 Patients also often have prominent autonomic findings and dry mouth is really common, it was present for the patient in our case and is something that we need to ask for if we're considering this. 02:36 We can also see other autonomic symptoms like constipation.
About the Lecture
The lecture Lambert Eaton Myasthenic Syndrome (LEMS): Overview by Roy Strowd, MD is from the course Disorders of the Neuromuscular Junctions.
Included Quiz Questions
Which of the following is not a characteristic of Lambert-Eaton myasthenic syndrome?
- Worsening of symptoms with muscle use
- Autoantibodies to presynaptic calcium channels leading to decreased ACh release
- Association with small cell lung cancer or less often lymphoma
- Proximal weakness (often proximal to distal)
- Areflexia (or hyporeflexia)
Author of lecture Lambert Eaton Myasthenic Syndrome (LEMS): Overview

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
This is a very clear and helpful review of LEMS
