Playlist
Show Playlist
Hide Playlist
Kidney Transplant – Renal Replacement Therapy

-
Slides Renal Replacement Therapy.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
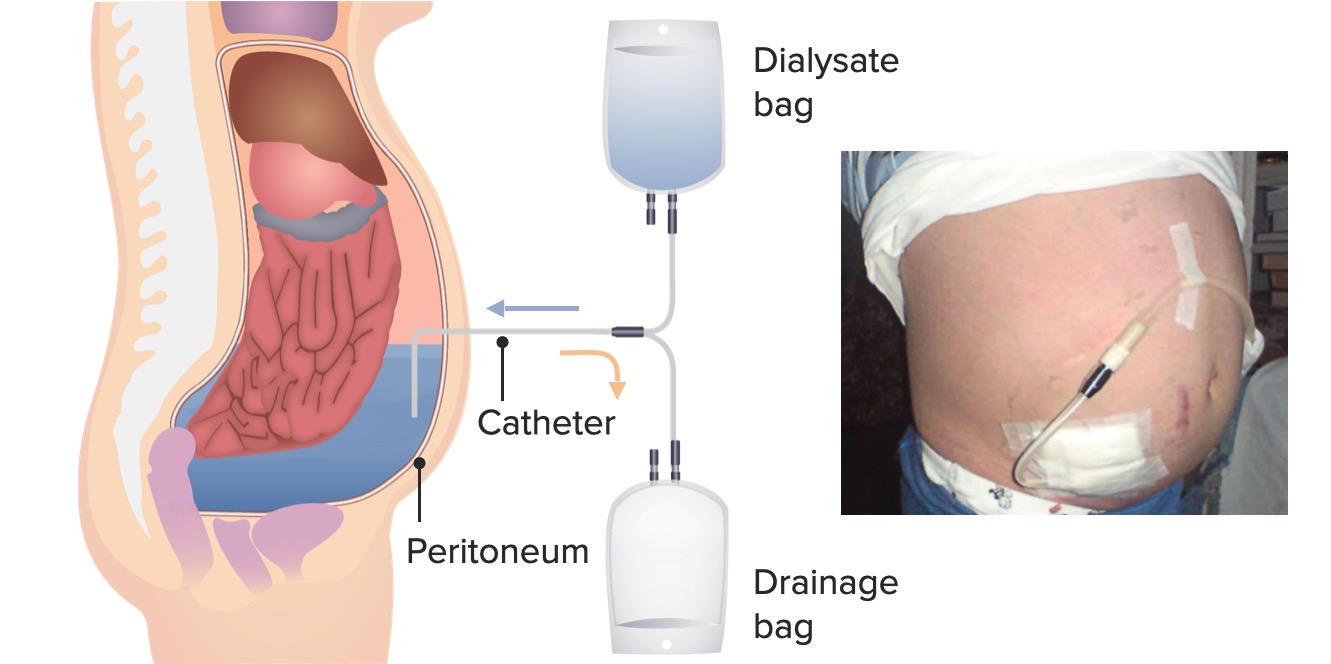
00:01 Finally, we talked about Kidney Transplant. 00:04 Again, that is my opportunity that I try to give every patient who's sitting before me. 00:08 Patients are eligible to be listed for transplant once their GFR falls below 20 mL/min. 00:14 So we don't have to wait for that patient to develop uremic syndrome. 00:17 We really want to start listing them, and talking about transplant when they're in that stage for chronic kidney disease. 00:24 Once they are deemed to be medically suitable and psychosocially suitable, then the patient can be listed or placed on the United Network of Oregon Sharing list (UNOS) And that means that they're eligible for a deceased donor. 00:39 Now, although they might be eligible and listed on UNOS, we always really strive to have a living donor for our patients. 00:46 And that living donor can either be related: it could be a father, a mother, a son, or a daughter, it could be a sibling. 00:52 Or it could be something that's unrelated: a partner, a friend, or an altruistic donor. 00:57 And in today's world with social media, we see more and more altruistic donors. 01:03 Something to think about living donation is that it provides a better outcome for our patients. 01:08 So we always encourage our patients and we encourage family members to think about living donation. 01:13 And something interesting, if you look at our slide here, when we do a kidney transplant, we actually don't need to remove the native kidneys. 01:21 We placed that transplanted kidney in the extra-peritoneal space. 01:27 So they essentially have three kidneys. 01:29 So it's actually quite interesting for our patients. 01:33 So again, if I have the opportunity to transplant my patient, I'm really going to go for a preemptive transplant. 01:39 That means if I can do a transplant before ever having them touch dialysis machine, that is going to give them the best survival advantage. 01:48 So I'm always looking to do that in my patient population. 01:52 I think what's most important when it comes to thinking about the different modalities of renal replacement therapy, is that you can't really approach it as a one size fits all or what's most convenient for you as the nephrologist or caretaker. 02:04 It really is a shared decision between the patient and their physician to decide what's best for them. 02:10 I have some patients, for example, like the gentleman here on the left, who's doing in-center hemodialysis. 02:15 They prefer to be in-center because they like the community. 02:19 They like the nurses, the technicians, they actually have friendships and relationships with the people who dialyze around them. 02:26 And that's a great source of comfort for them. 02:28 I have some patients who absolutely love home therapies like our lower image on the right. 02:35 So they love the fact that they can do peritoneal dialysis at home, or they can do some kind of home hemodialysis in the comfort of reading their own book, or doing homework, or it might allow them to actually work during the day and have a better life if they can dialyze every day. 02:51 And then finally, transplant which is our transplanted kidney that you can see at the top right corner. 02:57 Again, that allows people probably the best quality of life because they're not tied to a dialysis machine and they can live the life they want to on their own terms. 03:07 So with that, this concludes your lecture on renal replacement therapy.
About the Lecture
The lecture Kidney Transplant – Renal Replacement Therapy by Amy Sussman, MD is from the course Renal Replacement Therapy.
Included Quiz Questions
Which of the following is true regarding renal transplant?
- A preemptive transplant offers the best survival advantage.
- Patients are eligible for transplant only when they have developed uremic syndrome.
- Transplanting a cadaveric kidney offers the best outcome for the patient.
- The native kidney must be removed.
Patients with CKD are eligible for a kidney transplant at which of the following GFR thresholds?
- GFR < 20 mL/min
- GFR < 15 mL/min
- GFR < 50 mL/min
- GFR < 35 mL/min
- GFR < 40 mL/min
Author of lecture Kidney Transplant – Renal Replacement Therapy

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
