Playlist
Show Playlist
Hide Playlist
Kawasaki Disease (Mucocutaneous Lymph Node Syndrome)

-
Slides KawasakiDisease Pediatrics.pdf
-
Download Lecture Overview
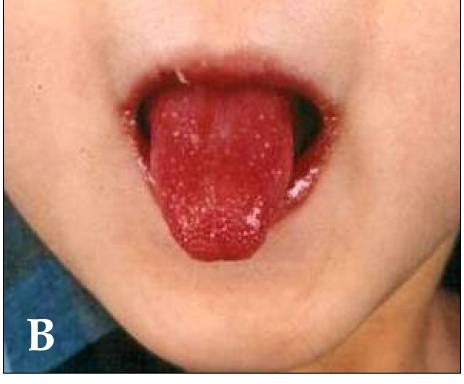
00:01 In this lecture we will discuss Kawasaki disease. 00:05 This is commonly addressed on multiple choice tests. 00:09 So Kawasaki's disease is a multisystem inflammatory condition of medium sized blood vessels. 00:16 The mechanism behind Kawasaki disease is not at all understood. 00:20 Nobody understands why this happens. 00:23 That said, there are some significant differences between Japanese and American Kawasaki disease, that might shed some light on the path of physiology. 00:33 The disease was discovered in Japan, hence the Japanese name. 00:38 Retrospective studies have been used to try and determine what was happening when we saw children who presented with coronary artery aneurysms. 00:48 They then looked at all these children who had all these symptoms prior to the development of the coronary artery aneurysms, and they put together a clinical criteria for the diagnosis of the disease. 01:00 That said, the Japanese disease and the American disease are so different that perhaps they are different diseases. 01:07 Children with Japanese Kawasaki tend to get much sicker and are much more likely to have giant aneurysms that can be life threatening. 01:16 These two diseases are treated differently on the two continents and we will focus in this lecture on American Kawasaki disease. 01:24 So Kawasaki is a common vasculitis in children. 01:28 80% of children will have it before five years of age. 01:32 However, a small percentage can have it even later, even over the age of ten. 01:38 It's a self-limited initial inflammatory stage that ends about after 12 to 14 days of significant inflammation. 01:49 However, if untreated during the inflammatory stage, that child now has a risk for development of coronary artery aneurysms, which can absolutely be life threatening. 02:01 In children under one year of age who have the disease, they will have a worse prognosis and be more likely to develop the coronary artery aneurysm. 02:11 So let's go through the clinical criteria for the diagnosis of this condition. 02:17 One way to remember it is crash and burn. 02:21 So burn first. 02:23 These patients need at least five days of fever. 02:27 Now let's go through the crash part of crash and burn. 02:31 Each letter in the word crash. 02:33 Stands for one of the five major criteria for Kawasaki disease. 02:38 C is for conjunctivitis. 02:40 This is a limbic sparing nonpareil and conjunctivitis or is for rash any type of rash. 02:48 A is for add in apathy, usually in the anterior cervical chain. 02:53 S is for strawberry tongue, but realistically, it can also be dry red cracked lips any sort of mouth mucous membrane changes and h is for hands and feet in particular. 03:04 Swelling, although peeling does also count as a criteria in that under one age group who have fever for seven days. 03:13 And no other explanation for it. 03:15 So for a diagnosis of Kawasaki, you need either four or five of these criteria. 03:21 Plus the five days of fever, the crash, four or five and the burn, you need five days of fever. 03:30 So the fever should be more than 37.5 degrees centigrade for at least five days. 03:37 If the patient meets other criteria, early treatment may be less effective. 03:42 And in general, one key thing about the systemic symptoms and this isn't a criteria, but it definitely tips you over the edge in these questionable cases. 03:52 Children with Kawasaki are irritable, they're fussy, they don't want you to be near them. 03:58 They are really fussy and they feel much better after their treatment. 04:03 Let's look at this conjunctivitis. 04:05 It'll look a little bit like this. 04:08 It's basically a non purulent red eye, no pus, just red. 04:13 And the area around the limbic parts of the iris is spared. 04:18 The redness is more peripheral, so it's limbic sparing. 04:22 And patients may have some photophobia, but that's not necessary at all for the diagnosis. 04:29 Oral mucous membrane changes include the strawberry tongue. 04:33 Can't really see it too well here, but this child definitely also has dry, red and cracked lips, which are positive pneumonic for the condition. 04:42 The lymphadenopathy is usually unilateral. 04:45 It's usually in the anterior cervical chain and they have to have one node that's at least 1.5 centimeters large. 04:54 The rash is nonspecific it's usually a macular popular erythematosus rash that looks like your typical viral exam them. 05:04 It usually involves the trunk the face, the extremities or the diaper area, the hands and feet condition, maybe red or just swollen. 05:15 Sometimes a patient comes in on day four of illness and the mom says, Oh yes, three days ago her hands were swollen and I just didn't do anything about it. 05:25 That counts. 05:27 A historical report of one of these findings counts in the criteria for this disease. 05:34 Here's an example of the peeling of fingers that can happen usually later in the syndrome. 05:41 Also, patients can get other symptoms which don't define the disease. 05:45 But do happen and may tip you over the edge in a questionable case. 05:50 Patients may develop an arthritis. 05:52 We may get lefties because patient can have a hepatitis. 05:57 Check for it by ultrasound. 05:59 Usually cases will resolve on their own. 06:01 However, surgical consultation may be indicated So here's a typical picture and it's a good picture to look at when these symptoms typically happen in the normal course of the illness. 06:15 From the top line, you can see that the fever will typically last more than five days. 06:20 It may last even to or weeks or longer, but eventually untreated that fever will resolve. 06:28 The other symptoms that we use to define the conditions such as the conjunctivitis. 06:34 The change in mucous membranes or the cervical lymphadenopathy tend to happen early in disease. 06:39 The rash perhaps a little bit later and the extremity change at first is swollen and then later is peeling. 06:48 Complications typically happen a little bit later on, such as the gallbladder high drops So radiologic studies and lab studies can be helpful, especially in a patient who is a typical Kawasaki Atypical Kawasaki is when patients meet either two or three criteria, and we need other findings to help justify whether or not we should be treating that patient. 07:16 Labs that are indicating that something more significant is going on include the ESR and the CRP They may have an elevated white count. 07:26 Patients on CBC may also have enormous acidic anemia. 07:31 This is consistent with just an inflammatory process. 07:34 Same thing with their thrombosis ptosis, which is a high platelet count. 07:40 Patients may have increased left vs that is a sort of systemic hepatitis from the inflammation. 07:49 One of the key things that shows up on test frequently is sterile diarrhea. 07:54 When obtaining a urinalysis on a patient. 07:56 With this, we may notice that they have increased white cells in their urine and suspect a urinary tract infection but nothing ever grows out. 08:05 One key, subtle point about the sterile pie area is it may be a urine arthritis rather than a pile of nephritis. 08:13 So if a patient is Kath arised to obtain the urine specimen, it may be missed. 08:18 These children should be bag urine and a urine culture should not be sent because bag urines have a higher false positive rate for a urinary tract infection. 08:30 Additionally, if for some reason the child does get a spinal tap, most do not. 08:36 A sterile CSF pleo ptosis is possible just like the sterile PI area Another key finding is low serum albumin. 08:44 They often have that as well. 08:47 So an echocardiogram is the mainstay of watching for these changes in their in their coronary arteries. 08:57 And we're looking for coronary artery aneurysms The echo may be positive early, but usually the coronary artery aneurysms are a later finding. 09:10 We obtain an echo around the time of diagnosis. 09:14 It's not a huge emergency, but we'd like to get it done in the first couple of days. 09:18 And the reason for that is not only are we looking for some rare signs of involvement of the heart, patients can get myocardial dysfunction or a pericarditis, or they can get very mild dilatation or activation of their corner arteries. 09:34 But mostly we're getting the early echo as a baseline for measurement of their coronary arteries. 09:40 So that we can compare their coronary arteries later on when they come back for follow visits. 09:46 And we're actually tracking for the development of an aneurysm Babies under six months of age with seven days of fever and no other symptoms at all, meet a typical criteria that is a special exception because very young infants with Kawasaki can present very typically the management of Kawasaki's is something you should be very familiar with after their five days of fever. 10:12 And once they've met criteria, four or five criteria for the typical Kawasaki disease or two or three criteria with additional lab findings and echo concerns, we will proceed to give IVIG. 10:27 This is high dose IVIG, which is two grams per kilo, and it's given over many hours. 10:34 It's given slowly because IVIG has side effects. 10:37 We worry about. 10:39 An example would be set shock. 10:42 Patients getting IVIG can have significantly lower blood pressures and go into shock. 10:47 So we're going to administer it very slowly. 10:50 Keep in mind there are some side effects of the IVIG that should concern you. 10:54 One of them is headache, and that's common But another concerning one is fever. 11:00 And this is because we're using a resolution of fever of the disease as a way of checking to see if the therapy is working. 11:08 If they continue to have fever. 11:10 We will wait typically a period of about 36 hours after the IVIG is completed to check for fever because an earlier fever may just be from the IVIG itself. 11:23 Additionally, we will give aspirin, we'll give high dose aspirin while they're in the hospital and in a febrile state. 11:30 And then once they're deferred vest and ready to go home, we will transition them to low dose aspirin. 11:36 The aspirin is given early as an anti-inflammatory and later as a way to prevent clots forming in the event that child does form a coronary artery aneurysm. 11:48 There is some evidence that the aspirin is of little benefit. 11:51 However, it's very unlikely this is going to change in the future because to do a study where you withheld aspirin would be hard to pull off. 12:00 Next, we will check these patients recurrently over a two to six week period every two to six weeks to make sure they're no longer having any involvement of their coronary arteries or that they're having none at all, or that if there is involvement we're tracking that involvement. 12:19 These children will get routine follow up echos until cleared by the cardiologist. 12:25 So that's my review of Kawasaki's disease. 12:28 Thanks for your time.
About the Lecture
The lecture Kawasaki Disease (Mucocutaneous Lymph Node Syndrome) by Brian Alverson, MD is from the course Pediatric Rheumatology and Orthopedics. It contains the following chapters:
- Kawasaki Disease
- Diagnosis of Kawasaki Disease
- Management of Kawasaki Disease
Included Quiz Questions
Which of the following is a life-threatening complication of Kawasaki disease if not treated in the inflammatory stage?
- Coronary artery aneurysm
- Renal failure
- Arthritis
- Gallbladder hydrops
- Hepatitis
Which of the following is not a diagnostic criterion for Kawasaki disease?
- Irritability
- Conjunctivitis
- Adenopathy
- Rash
- Strawberry tongue
Which of the following is NOT a characteristic of the rash seen in Kawasaki disease?
- Petechiae
- Erythematous
- Maculopapular
- Looks like viral exanthema
- Involves the trunk, face, extremities or diaper area
Regarding Kawasaki disease, which of the following appears later in its course?
- Skin peeling
- Fever
- Conjunctivitis
- Rash
- Strawberry tongue
Which of the following lab results would be expected in a patient with Kawasaki disease?
- Elevated ESR, elevated CRP, leukocytosis, elevated LFTs
- Elevated ESR, elevated RBC, elevated LFTs
- Thrombocytosis, elevated CRP, leukopenia
- Leukopenia, thrombocytopenia, elevated LFTs
- Elevated LFTs, decreased hemoglobin, leukopenia
Which of the following is NOT true regarding the management of Kawasaki disease?
- ASA is not necessary for the early stages.
- Follow up echocardiograms every 2-6 weeks to check coronary arteries
- Supportive treatment
- Give high dose IV immunoglobulin at 2 g/kg
- The IV immunoglobulin has to be given slowly over many hours
Which of the following is a finding expected in the cerebrospinal fluid of patients with Kawasaki disease?
- Sterile pleocytosis
- High sugar
- High protein
- High RBCs
- Low albumin
Author of lecture Kawasaki Disease (Mucocutaneous Lymph Node Syndrome)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Is a good review of the disease, focused on what's important
Excellent lecture. A typical major pediatrics topic. Mnemonic is very useful along all the comments. Thanks!
