Playlist
Show Playlist
Hide Playlist
Kawasaki Disease

-
Slides Inflammatory Vascular Diseases.pdf
-
Reference List Vascular Medicine.pdf
-
Download Lecture Overview
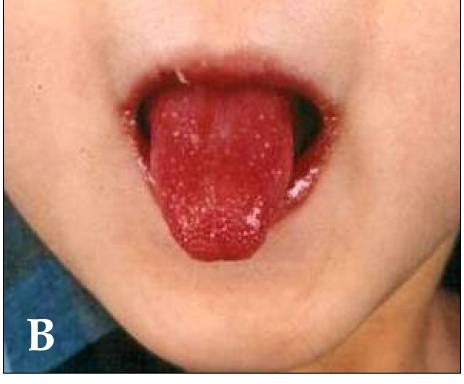
00:00 Let's move on now to a very, uh, unusual syndrome that affects very small children, but also does medium-sized arteries. 00:10 So this is in the same category as with polyarteritis. 00:15 Um, it is medium-sized arteries that are involved, but in very small children. 00:19 It's a disease that's actually almost only seen in Japan or very rarely in the West. 00:26 Um, it, uh, is associated with a specific clinical picture that I'm going to show you, actually some pictures of it. 00:34 Um, but there's of course, a very, uh, there's evidence of inflammation because there's an elevated erythrocyte sedimentation rate. 00:41 There's elevated CRP, um, there's elevated white count. 00:45 The patients are often anemic. 00:47 And again, the biopsy, um, demonstrates characteristic medium-sized vessel involvement. The coronary arteries are commonly involved. 00:55 And if not treated, this can go on to lead to aneurysms that can even show up in adults. 01:01 They don't go away. 01:03 Again. The treatment is either um uh, high dose intravenous gamma globulin, immunosuppressive agents such as glucocorticoids, um, and in fact, this can be fatal uh, in children. 01:19 Um, so um, again, it occurs very frequently in Japan, often, um, associated with congenital heart disease and for some reason more common in boys than in girls and almost always in children who are less than five years of age. 01:32 It is thought to be an autoimmune disease, but staph aureus infections can be involved. 01:38 Um, and as I said, the coronary arteries can be involved with aneurysm formation in anywhere from 15 to 25% of patients. 01:46 It affects not only arteries, but also mucous membranes and lymph nodes, and is sometimes called mucocutaneous lymph node syndrome. 01:56 Um, often the fevers are quite high above 102 and they don't disappear with Tylenol. 02:02 Again. Therapy, I.V. 02:04 gamma globulin, high dose aspirin. 02:07 Um, and usually there's a significant improvement when patients are given IV gamma globulin. Um, there are no blood tests that are specific for it. 02:16 Um, usually the diagnosis is made on clinical grounds. 02:20 And here we just see a little diagram with a picture of all of the forms of, of clinical expression. Um, this is an example of a 12-month-old Japanese male admitted with a very high fever, lasted for five days, not responded to Tylenol or ibuprofen. 02:37 He has extremely red eyes without pus or drainage. 02:41 He has bright red, chapped lips. 02:43 Um, there's red mucous membranes in his mouth. 02:46 His tongue is red and has little bumps like a strawberry, so-called strawberry tongue, the palms of the hands and the and the flat, uh, soles of the feet, um, also can be red and there can be skin rashes. 03:01 And the diagnosis is made by biopsy. 03:04 Um, and again, it involves medium sized arteries and the treatment is immunosuppression.
About the Lecture
The lecture Kawasaki Disease by Joseph Alpert, MD is from the course Inflammatory Vascular Diseases.
Included Quiz Questions
Kawasaki disease is most common in which of the following countries?
- Japan
- Germany
- Argentina
- China
Kawasaki disease is most prevalent in which of the following countries?
- Japan.
- Indonesia.
- Malaysia.
- Thailand.
- Sierra Leon.
Which of the following is most likely to be seen during an oral examination in a patient with Kawasaki disease?
- Strawberry tongue.
- Geographic tongue.
- Black tongue.
- Hairy tongue.
- Bleeding tongue.
Author of lecture Kawasaki Disease

Joseph Alpert, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
