Playlist
Show Playlist
Hide Playlist
Cystoisospora – Protozoa (GI Infection)

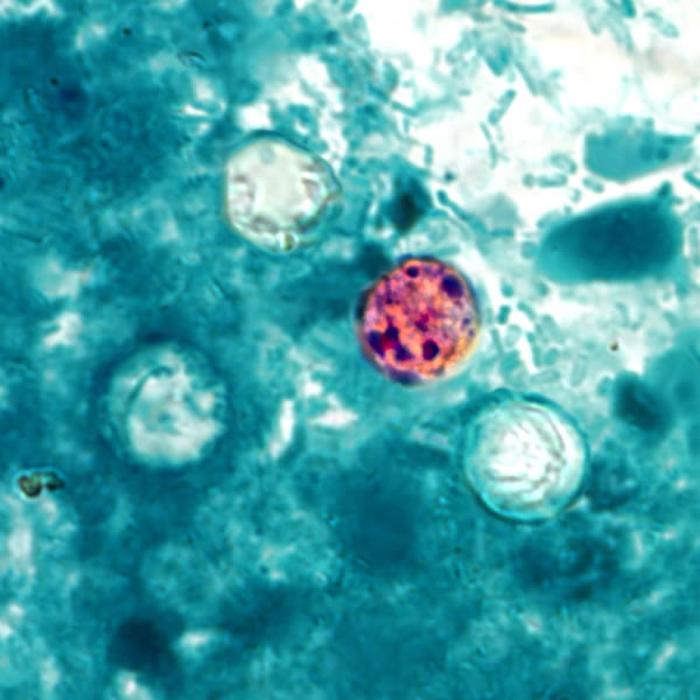
00:01 Cystoisospora is the official name of this intestinal parasite, but it is still commonly called by its older name, Isospora. 00:08 Cystoisospora comes from the genus of the Sarcocystidae family. 00:12 It is a coccidian parasite which produces a large oocyst about 25 microns in diameter, with a typical ellipsoidal shape. 00:21 It can best be seen with an acid fast stain performed on a fecal smear. 00:25 The pictures in front of you show the classic appearances of a coccidian parasite, encysted in a firm outer shell or wall. 00:33 The cystoisospora go through classic developmental stages, which we'll discuss shortly, each of which has a possible contribution to the clinical pathogenesis. 00:42 Transmission, as we're seeing with most parasites, is via fecal-oral spread of the oocysts from contaminated water. 00:49 Incubation after ingesting an oocyte is approximately one week, and the typical human pathogen which we are most concerned about is Cystoisospora belli. 00:59 Let's look now then at the mechanism of pathogenesis. 01:03 And as with other water-associated parasites, there is at first an ingestion stage, a processing stage through the gut, and then an eventual departure from the gut of recreated oocysts, which can either infect others or certainly contaminate a water supply. 01:21 However, the primary infection that the first sign of inflammation occurs when the oocysts are ingested and break down into the first stage, which attaches to the brush border of the small intestinal mucosa. 01:37 Let's look at that a little bit more closely. 01:40 Having ingested the oocyte, it sort of exists itself and releases sporozoites which attach to the brush border of the intestinal epithelium, as you can see in this slide. 01:52 The sporozoites are then inserted into the cytoplasm of the cell where they undergo asexual replication to create merozoites. 02:03 After the merozoites are created, they rupture through their host cells, which is the first sign of inflammation and a triggering of the human immune response. 02:15 This allows for malabsorption, petechial hemorrhages, and sort of a chronic scarring of those affected cells, leading to villous atrophy and crypt hypertrophy. 02:27 Next is the sexual reproduction stage, and so that merozoite reenters another host cell. 02:35 So this is an autoinfection stage. 02:38 Infection reoccurring within the lumen of the gut. 02:41 And then goes through sexual maturation to then create a gamont. 02:46 And then to release a fully formed cyst into the stool. 02:51 Again a rupture, a lysis of the host cell occurs, leading potentially to even further inflammation. And all the results, as we just talked about after the asexual stage. 03:04 So how this looks clinically then is the patient will develop non-bloody diarrhea non-bloody because it's usually the intestinal epithelial cells, not the vasculature, which are being ruptured in this case. 03:18 However, because this will affect the actual intestinal wall, there may be abdominal pain related to that. Certainly there will be fever associated with this ongoing repetitive re- or auto-inoculation stages of inflammation. 03:35 Then the malabsorption is probably the more prominent part of isospora belli's infection malabsorption. Because the cells are unable to retain or absorb water and other nutrients, so patients may become severely dehydrated. 03:50 They certainly can also have associated weight loss. 03:54 And for patients who are chronically infected, such as infants or immunosuppressed patients, they have a malabsorptive syndrome and may have failure to thrive or failure to gain weight as their presenting symptom. 04:08 Diagnosis is by demonstrating the oocysts in stool and again, as you saw in the very first image, it's a characteristic coccidian appearance of the oocyst. 04:18 Treatment then, especially for those who are immunocompromised, are very young, is with a sulfonamide, especially trimethoprim sulfamethoxazole. 04:27 So isospora and Isospora belli are the classic pathogens in this case. 04:32 And they're a very typical sort of, uh, sexual and asexual maturation cycle as seen in the coccidian parasites. 04:41 Remember them well, you'll see this pattern repeat in other typical and similar parasites.
About the Lecture
The lecture Cystoisospora – Protozoa (GI Infection) by Sean Elliott, MD is from the course Parasites.
Included Quiz Questions
Which of the following stages of the Cystoisospora life cycle, when ingested by an individual, causes an infection?
- Oocyst
- Sporocyst
- Merozoite
- Schizont
- Gamont
Which of the following species of Cystoisospora is most commonly implicated in the manifestation of acute, non-bloody diarrhea?
- C. belli
- C. ohioensis
- I. buteonis
- I. felis
- C. suis
For a patient having clinical manifestations following ingestion of Cystoisospora oocysts, which of the following is the pharmacological agent of choice?
- Trimethoprim-sulfamethoxazole
- Metronidazole
- Tinidazole
- Azithromycin
- Nitazoxanide
Author of lecture Cystoisospora – Protozoa (GI Infection)

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
