Playlist
Show Playlist
Hide Playlist
Intussusception

-
Slides GIP Intussusception.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
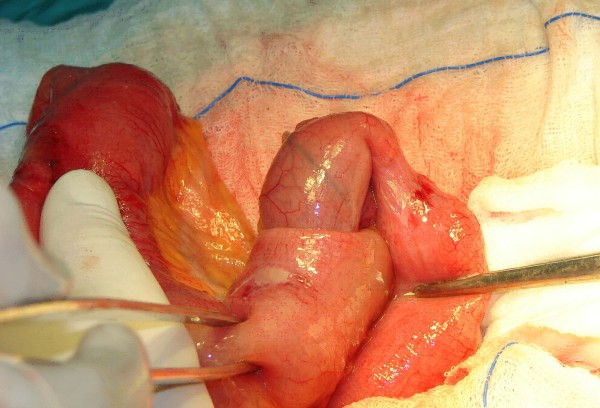
00:00 Welcome. In this talk, we're going to be covering the topic of intussusception. 00:05 What is this? Well, it's a telescoping of one part of the bowel into the adjacent bowel. 00:11 And most commonly, this is going to be from the proximal bowel into the more distal bowel because that's the way the peristalsis is carrying all the contents, including the bowel wall. 00:22 What is being demonstrated in the picture here is intussusception of the terminal ileum into the cecum but any part of the bowel can have it, have this particular telescoping occur The epidemiology of this is interesting. 00:39 It's not super-duper common but about 30 out of 100,000 live births will have this. 00:45 Now, this is saying, "Oh, this is congenital intussusception. Correct. There can also be intussusception that occurs at later years of life. 00:54 In the early newborn period is the most common cause of bowel obstruction and 60% of cases of kind of pediatric intussusception will be identified within the first year of life. 01:08 The pathophysiology. In the vast majority of cases, we haven't a clue. 01:13 We don't know what caused the bowel to be drawn into the other part is most commonly in the children. 01:19 Idiopathic is relatively rare in adults where we often will have an etiology. In terms of causes, infection is one. 01:29 If we have an enlarged Peyer's patch, typically, in the distal ileum, those large Peyer patches can be a point of traction with stool and peristalsis carrying that into the next segment of bowel. 01:41 So an upper respiratory tract infection may be a predicate for developing that cause of intussusception. 01:49 And bacterial inflammation of the bowel and enteritis can also be a cause. 01:54 Other pathologies that can be associated with this. Meckel's diverticulum is actually one of the more common in children. 02:01 And in a separate talk, we will discuss Meckel's diverticulum, so, I won't go into detail here. 02:06 Suffice to say, it's an outpouching of the small bowel, usually, within about 10 centimeters of the ileocecal junction. 02:13 Henoch-Schonlein purpura will cause thickening of the bowel mucosa and that can be a point of traction. 02:20 Lymphoma by causing bowel nodules of lymphoid tissue to expand can be a cause or intestinal polyps or tumors and this is actually the most common etiology in adults where a polyp will be caught and dragged along by fecal material and pull it up into the next segment of bowel from proximal to distal. 02:42 This is just showing you a segment of bowel, again, we're looking at the terminal ileum as it dumps into the cecum. 02:48 The little thing sticking down is the appendix and with traction for whatever reason, for all the things that we've talked about, that gets pulled up into the distal or into the proximal cecum. 03:00 When that happens, now, you may actually have partial obstruction because we have two parts of bowel, one inside the other. 03:07 The bowel made the bowel circulation, the vasculature may be compromised because of that pulling up in there and twisting and turning of that. So, we may get focal ischemia. 03:18 We may end up with constipation. There are a variety of symptoms we'll talk about in the next part of the talk. 03:24 So, in terms of clinical manifestations, a sudden onset of cramping, severe intermittent abdominal pain can be a presentation turned on its head. Just because you have cramping, severe abdominal pain that comes on all of a sudden doesn't mean that you have intussusception. 03:41 Vomiting, an apparent mass, you know, parts of the bowel inside another part of the bowel may cause a focal expansion. 03:48 Blood in the stool due to ischemia, constipation because you can't get anything passed that point of telescoping. 03:56 These are all things that can be associated with it. They are not specific to intussusception. 04:01 So, how do we make the diagnosis? Well, a clinical history of acute onset of pain. 04:07 There may be an apparent mass. Doesn't have to be. There may be abdominal distention. 04:13 So, more proximal bowel not able to move its contents more distally may dilate. 04:19 There may be signs of peritonitis, inflammation of the peritoneal lining. So, rebound tenderness or guarding. 04:25 But that's all only usually near the end of the story. And you may have high-pitched bowel sounds as the bowel tries to squeeze through there. 04:34 You may have little bits, jets of gas that get heard through a stethoscope as high-pitched. 04:40 Imaging can be helpful if you happen to get exactly the right image. This is on an ultrasound and we're seeing a target sign. 04:48 So, what you're looking at is an outer rim of bowel. And then, you have an inner telescoping of small bowel. 04:55 I believe that this is actually at the cecum. And management, overall, when we have made the diagnosis. 05:02 So, in some cases, this will resolve spontaneously and we're good to go. 05:10 It may recur though if there is a polyp, if there is lymphoid tissue expansion, etc. 05:17 We need to give the patient fluid resuscitation. 05:21 They will probably be somewhat dehydrated as a combination of not eating but also, the inflammation at that segment of bowel is causing edema and loss of fluid within the vascular system. 05:33 You'll want to decompress the upper and lower bowel. So, you'll do nasogastric decompression, put in an NG Tube. 05:41 An enema or sigmoidoscopy may actually relieve intussusception by pushing it back the other way. 05:47 And then, maybe a treatment for little kids who have a much more distal sigmoid intussusception. 05:54 And then, if we can't reduce it by any of those other mechanisms, we will result to surgery. And with that, intussusception.
About the Lecture
The lecture Intussusception by Richard Mitchell, MD, PhD is from the course Small and Large Intestines Disorders.
Included Quiz Questions
What defines intussusception?
- Telescoping of one part of the bowel into the adjacent bowel
- Wrapping of the bowel around the adjacent bowel
- Mucosal ulceration and erosion
- Disordered peristalsis
- Outpouches of capillaries prone to bleeding
Which age group is most commonly affected by intussusception?
- 6–36 months old
- 5–7 years old
- 3–4 months old
- 10–20 years old
- 60–80 years old
What is the most common mechanism of intussusception formation?
- Idiopathic
- Parasitic infection
- Bacterial infection
- Inflammatory bowel disease
- Internal hemorrhoids
Author of lecture Intussusception

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
