Playlist
Show Playlist
Hide Playlist
Intussusception: Management

-
Slides Intussusception Surgery.pdf
-
Download Lecture Overview
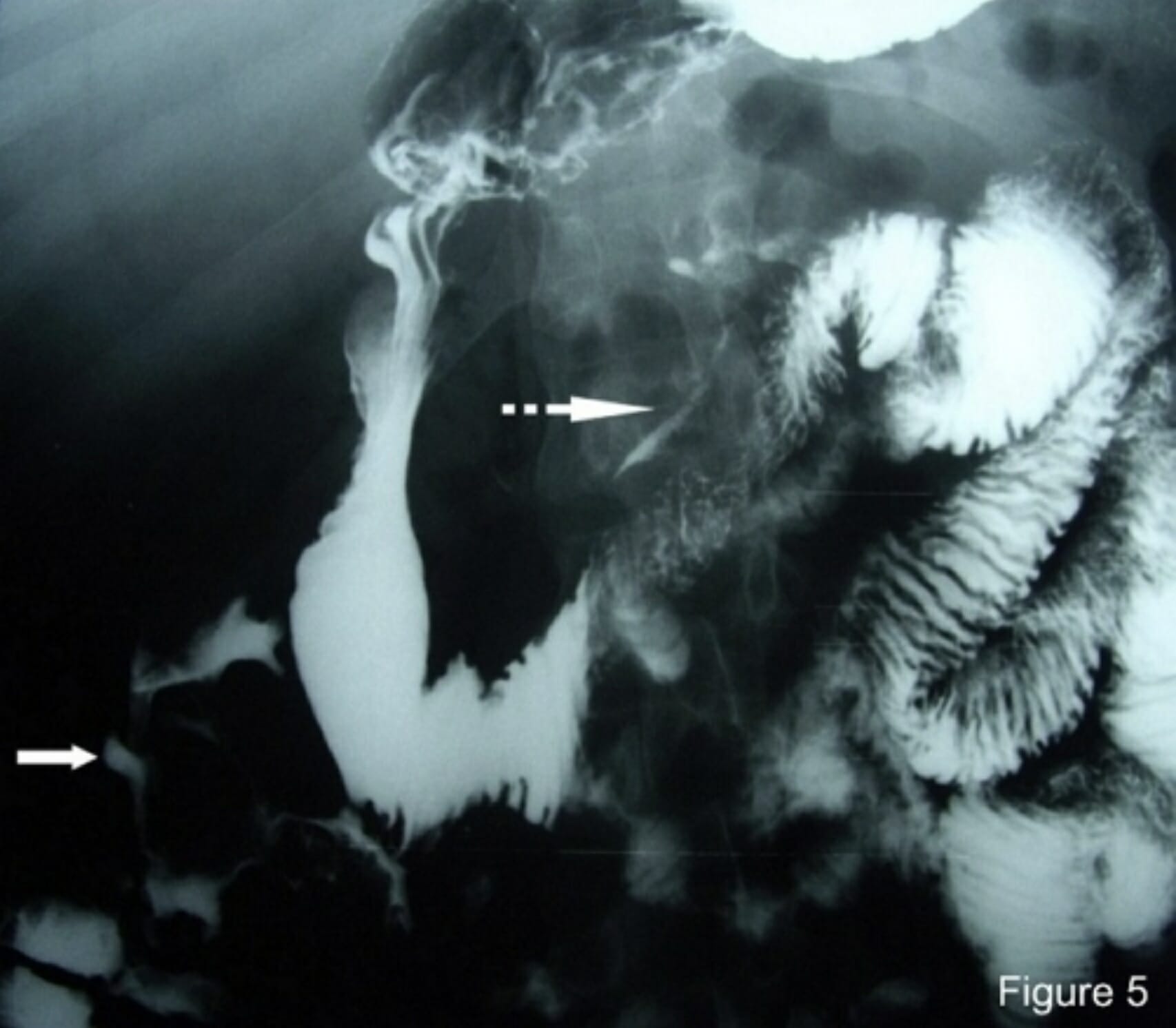
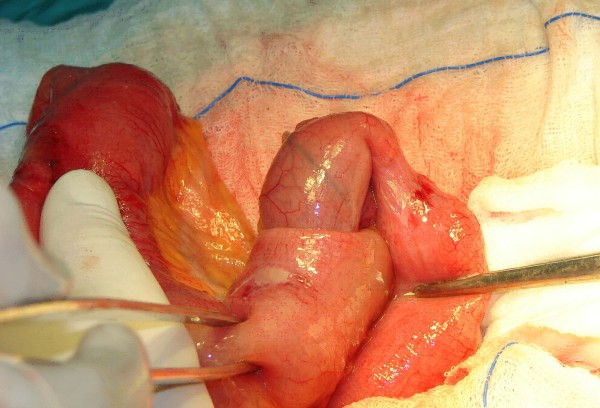
00:01 Although some patients may require surgery, particularly with signs of ischemia or perforation, the vast majority of patients respond quite well to non-operative reduction. 00:12 There are a couple of options. 00:15 There's therapeutic enemas. 00:17 This is a hydrostatic reduction where a column of barium is inserted into the rectum at a certain height. 00:23 This height is optimized to both reduce the intussusception, but also to minimize the risk of perforation. 00:30 This can be performed hydrostatically with either contrast barium or water-soluble contrast. 00:36 Similarly, pneumatic or air enemas have increasing use in patients with reduction of intussusception. 00:44 There's no need for barium in this situation. 00:47 Both have fairly good success. 00:50 Please also keep in mind, this is not as useful if it's not ileocolic. 00:56 In any other portions of the intestines, pneumatic or therapeutic hydrostatic enemas may not be able to reduce the proximal of the section. 01:03 It is worth mentioning that in 10% of cases, intussusception recurs after reduction. 01:08 Now, in this situation where patients do not reduce intussusception with the enemas therapy, there are some indications for surgery. 01:22 For example, if the patient develops peritonitis, remember, in babies, they may not be able to present with classic findings of peritonitis as in adults. 01:32 Everything generally just hurts. 01:34 But if you find that there is discoloration of the skin, this may be a sign of peritonitis. 01:40 Next, pneumoperitoneum. 01:43 This suggests likely perforated. 01:45 Although you don't know where the perforation is, this is an absolute indication for surgery. 01:51 And lastly, as is in the case with most kids, progressive clinical deterioration. 01:56 As a reminder, if a clinical scenario is presented to you and the patient has suspicion for ischemia or clinical deterioration, I strongly recommend that you go to the operating room. 02:08 In the operating room, this is how we take care of intussusceptions. 02:14 Generally, it's recommended that you push the invaginated segment out rather than pulling it out. 02:21 This reduces the perforation risk. 02:23 It’s common physics. 02:25 If you're successful or not successful, management is a little bit different. 02:31 If you're able to reduce intussusception in children by simply pushing out the invaginated segment and the segments appear viable, then complete the procedure by doing an appendectomy. 02:45 However, if you are not easily able to reduce intussusception, it’s probably safer to perform a segmental resection. 02:54 Let's review some very important clinical pearls and high-yield information. 02:59 In patients who do not succeed an enema reduction, they can be repeated. 03:05 Additionally, if a patient initially succeeds with enema reduction and re-intussuscepts, they’re also a candidate for enema reduction as long as these patients do not demonstrate any signs or indications for surgery that we've discussed. 03:22 And for your examination, remember, lead points are rare in children. 03:28 Lymph nodes, however, is the most common lead point, usually following upper respiratory infection. 03:34 However, if an intussusception is presented in an adult patient, think about cancer as most patients - adult patients with intussusception have a lead point to explain why they develop a non-idiopathic non-ileocolic intussusception. 03:53 Let's talk about Meckel's Diverticulum This is a small congenital diverticular of the small intestines that often finds its way onto tests. 04:01 It is often described as following the rules of 2's meaning it occurs in 2% of the population, but only 2% of those patients develop symptoms. 04:10 Usually it is two inches in length, normally located within two feet of the ileocecal valve. 04:17 And commonly symptomatic in children less than two years of age. 04:20 The symptoms include abdominal pain, bowel obstruction, bleeding and intussuspection if the diverticular inverts into the bowel lumen. 04:29 Thank you very much for joining me on this discussion of intussusception.
About the Lecture
The lecture Intussusception: Management by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Which of the following types of intussusception is MOST likely to benefit from barium enema and pneumatic reduction?
- Ileocolic
- Ileoileal
- Ileo-ileo-colic
- Colocolic
- Retrograde
Which of the following is NOT an indication for surgery for intussusception?
- Absence of sepsis
- Peritonitis
- Perforated intestines
- Pneumoperitoneum suggesting vascular compromise
- Unstable patient
Author of lecture Intussusception: Management

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
