Playlist
Show Playlist
Hide Playlist
Surgery: Intestinal Malrotation

-
Slides IntestinalMalrotation Surgery.pdf
-
Download Lecture Overview
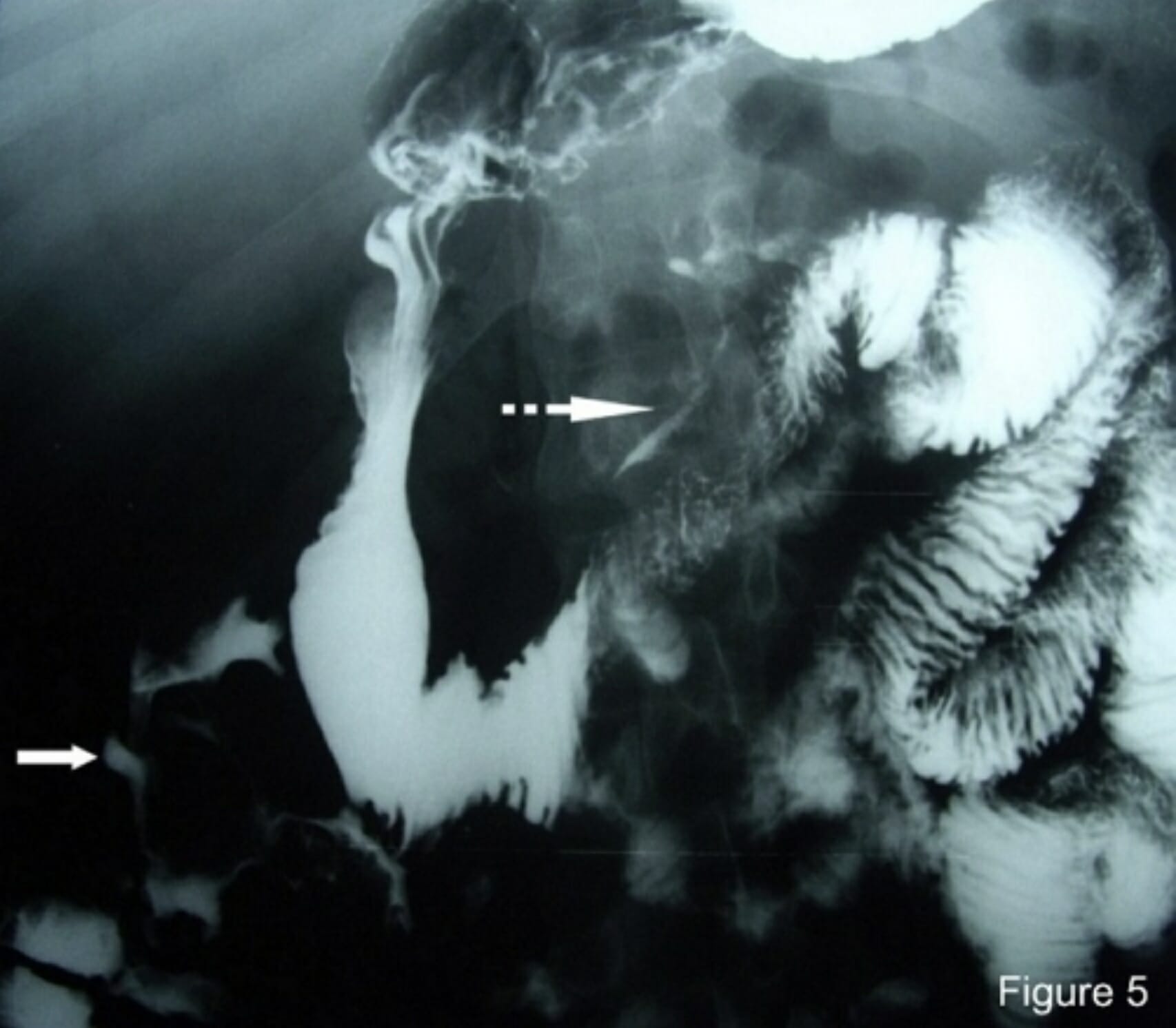
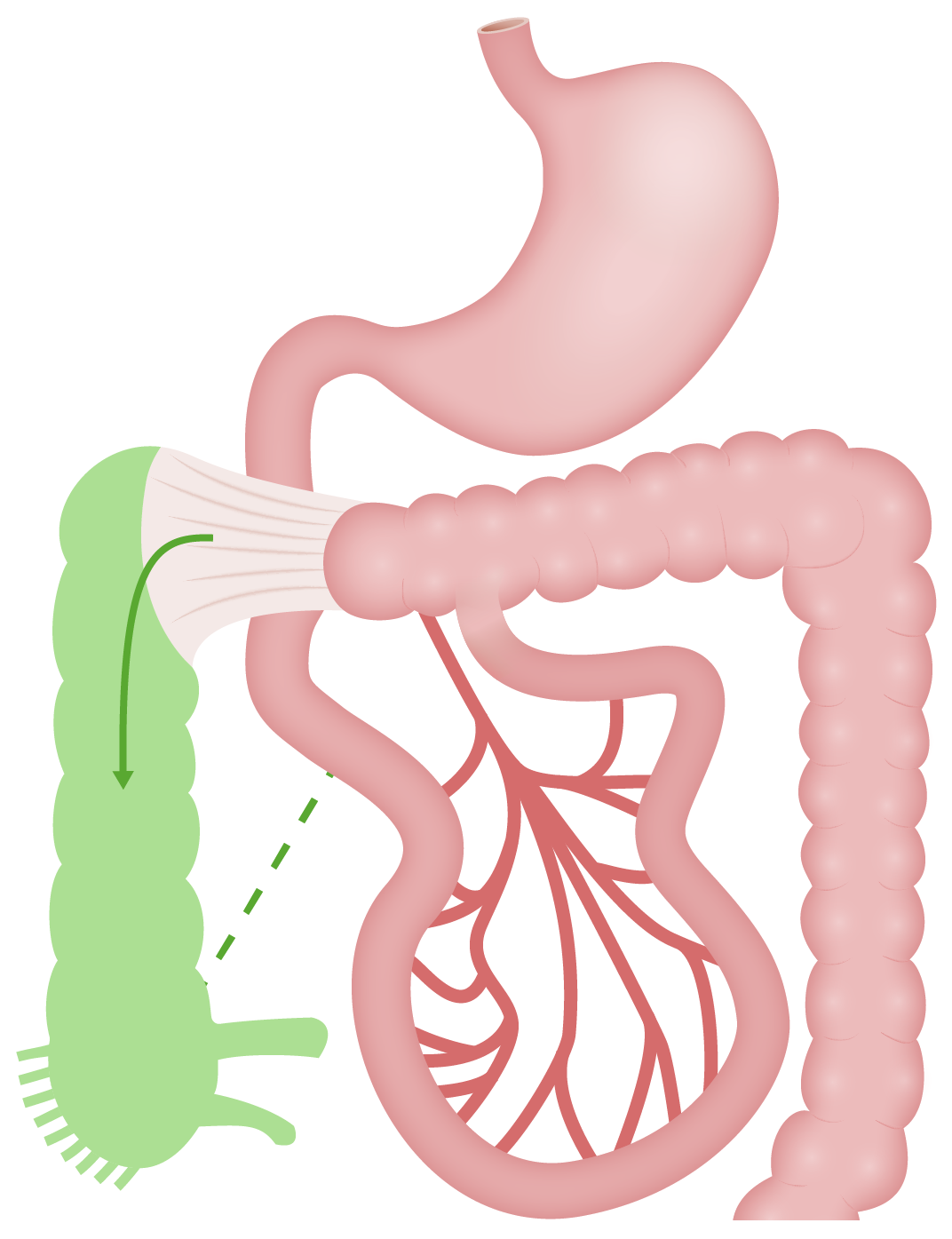
00:01 Welcome back. 00:02 Thanks for joining me on this discussion of intestinal malrotation in the section of pediatric surgery. 00:11 Let's visit the embryology of the GI tract. 00:14 The GI tract (or gastrointestinal tract) is usually divided into three segments. 00:19 Embryologically, they represent the foregut, the midgut and the hindgut. 00:26 The foregut is generally proximal to the ligament of Treitz. 00:34 For embryologic reasons, the GI tract needs to herniate out of the abdominal cavity. 00:41 That's because there's not enough room for the rotation to occur inside. 00:45 When the GI tract herniates out, it actually rotates 270°. 00:52 And the duodenojejunal junction and the cecal attachments form after the rotation and subsequent reattachment into the abdomen. 01:02 This is what we know as a normal rotation. 01:07 However, a malrotation, as you see on the right side of the screen, duodenojejunal and cecal attachments do not occur in the normal places. 01:20 Midgut volvulus generally presents itself as bilious emesis, diffuse abdominal pain and usually a surgical emergency. 01:29 That makes sense. 01:30 When the intestines are twisted on itself, it can actually cut off its blood supply. 01:35 In this surgical image, you notice that the bowel proximal and distal to the loop of volvulus is actually distended. 01:46 What would the babies look like and their classic physical findings? Babies may have distended abdomens. 01:54 There may be skin discoloration if it's late. 01:56 Again, when there are ischemic bowel changes, the skin may actually turn a little bit red. 02:02 And babies may actually have guarding and drawn up knees. 02:06 Unlike in other infantile small bowel obstructions, malrotation is considered a surgical emergency and it's usually in babies who are a little bit older. 02:18 What might you find on routine laboratory? In a chemistry, you could find low sodium, low chloride and low bicarb. 02:27 And on a CBC, one might find an increased white blood cell count or leukocytosis. 02:35 Here are some representative abdominal x-rays demonstrating potential findings of malrotation. 02:41 Unfortunately, like other small bowel obstructions, malrotation may demonstrate itself on abdominal x-rays simply as distended loops, as you see on the right side of the screen. 02:54 Upper GI series are incredibly helpful. 02:57 Upper GI series, such as this one and this one, demonstrate the abnormal attachments of the duodenal junction as well as the cecum. 03:09 In these series, you will notice that the duodenal junction is on the right side of the spine as opposed to the left side. 03:16 Remember, the ligament of Treitz in normal anatomy is on the left side of the spine.
About the Lecture
The lecture Surgery: Intestinal Malrotation by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Which of the following abnormalities is seen on routine laboratory tests in cases of malrotation with midgut volvulus?
- Hyponatremia
- Leukopenia
- High chloride
- Hypokalemia
- High bicarbonate
Which of the following diagnostic techniques is the modality of choice for evaluating intestinal malrotation?
- Upper gastrointestinal series
- Ultrasound of the abdomen
- Barium swallow
- MRI abdomen/pelvis
- Plain radiograph of the abdomen
Author of lecture Surgery: Intestinal Malrotation

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Explained very well in detail, all components or the topic are covered very clearly
