Playlist
Show Playlist
Hide Playlist
Infectious Esophagitis

-
Slides GD Esophagus.pdf
-
Download Lecture Overview
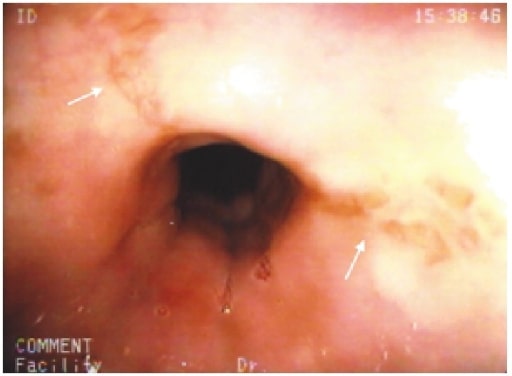
00:01 Let’s take a look at infectious esophagitis. 00:03 We’ll begin by looking at viruses. 00:05 The usual suspects: CMV, Herpes, Varicella, HIV. 00:12 In the esophagus, look for an immunocompromised patient. 00:16 Fungal: Candida being the most prevalent here, immunocompromised patient. 00:21 Bacterial: something like a Beta-hemolytic streptococci such as Pyogenes. 00:28 CMV Esophagitis will be our first discussion. 00:31 Immunocompromised patient is, or immunocompromised host, is the patient that you’re dealing with. 00:38 Reactivation of latent infection. 00:40 Remember with viruses, if the patient becomes immunocompromised, there’ll be reactivation of it. 00:47 Concurrent disease in the retina, liver and lungs. 00:49 Whenever you have these viral infections, or infections in general, and if esophagus is involved and you know your patient is immunocompromised, very likely there would be other organs involved including, you’ve heard of retinopathy with CMV. Or retinitis, liver, lungs involved. 01:09 Endoscopy is the test of choice, serology for CMV not helpful, CMV PCR may be positive. 01:19 Polymerase chain reaction might be positive so that you can identify your patient with CMV. 01:26 Whenever there is infectious esophagitis, now apart from maybe dysphagia, there’s going to be painful swallowing - odynophagia. 01:36 Sub-sternal chest pain and a viral infection, a low grade type of fever. 01:43 Endoscopy, you want to pay attention to description here. 01:46 It’s a well circumscribed ulcer with normal mucosa surrounding it. 01:53 What we’ll do here, so that you know as to what to expect and what to compare this to, would be HSV esophagitis. 02:00 So Cytomegalovirus esophagitis, you’d find this ulcer to be circumscribed and rather larger when compared to upon endoscopy, a HSV or Herpes type of esophagitis, where there you’d find crops of vesicles. 02:18 The biopsy shows viral inclusions, has been more specific for CMV immunostains. 02:24 The viral tissue culture, not sensitive and Foscarnet may be necessary for resistance. 02:30 Foscarnet. 02:32 Acyclovir, Gancyclovir, Foscarnet - drugs that you want to keep in mind in the family of Herpes. 02:40 Management, it would in fact be your IV ganciclovir followed by something like Valgancyclovir and Foscarnet if you’re thinking about your refractive cases that we just mentioned. 02:53 On endoscopic examination of CMV, remember that your patient most likely immunocompromised. 02:58 How? Maybe taking drugs or maybe perhaps even, you’re thinking about HIV status. 03:05 You’ll notice here, couple things that I wish to point out to you. 03:09 We’ve looked at a bunch of upper endoscopic pictures, we’ve looked at rings, looked at strictures, we looked at cancers of esophagus, we looked at Barrett’s. 03:20 Here, you’ll notice the following. 03:24 Here we have a focal region of ulceration taking place with the surrounding area which is relatively normal. 03:32 I want you to focus on normal. 03:35 There’s no narrowing of the lumen, the caliber of the esophageal lumen has not been compromised. 03:41 I do want you to pay attention to the blood vessels that are passing in the lining of the esophagus. 03:48 This is all perfectly normal. 03:50 At some point of time, you will be responsible to identify esophageal varices secondary to portal hypertension. 03:57 And you’ll notice at that point, that the bulging of the esophagus will be taking place as you would expect with varices. 04:04 Here, none of this is present and I need you to get more and more comfortable with upper endoscopy so that you’re able to identify, lesions just like that. 04:17 This is CMV esophagitis.
About the Lecture
The lecture Infectious Esophagitis by Carlo Raj, MD is from the course Esophageal Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
A 55-year-old man who is HIV-positive comes to the office complaining of severe pain and discomfort in his throat for the past few weeks. What would be the MOST likely endoscopic finding in this patient?
- Well-circumscribed ulcers surrounded by normal mucosa
- Stricture formation near the lower esophageal sphincter (LES)
- Barrett's esophagus
- Necrosis
- Adenocarcinoma
Author of lecture Infectious Esophagitis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Thank you. I´m going to present this topic at my hospital.
