Playlist
Show Playlist
Hide Playlist
Hypokalemia: Clinical Manifestations

-
Slides Potassium Disorders Hypo and Hyperkalemia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
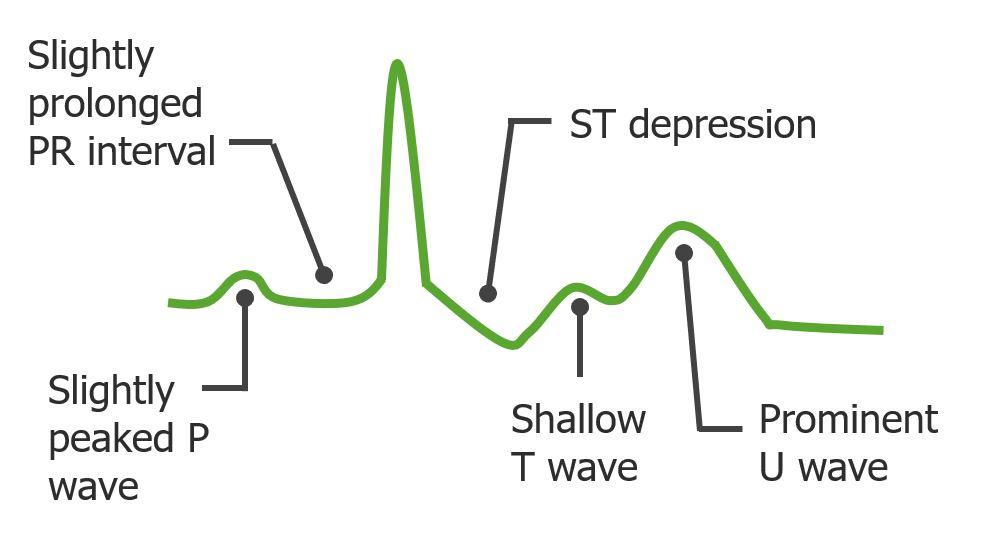
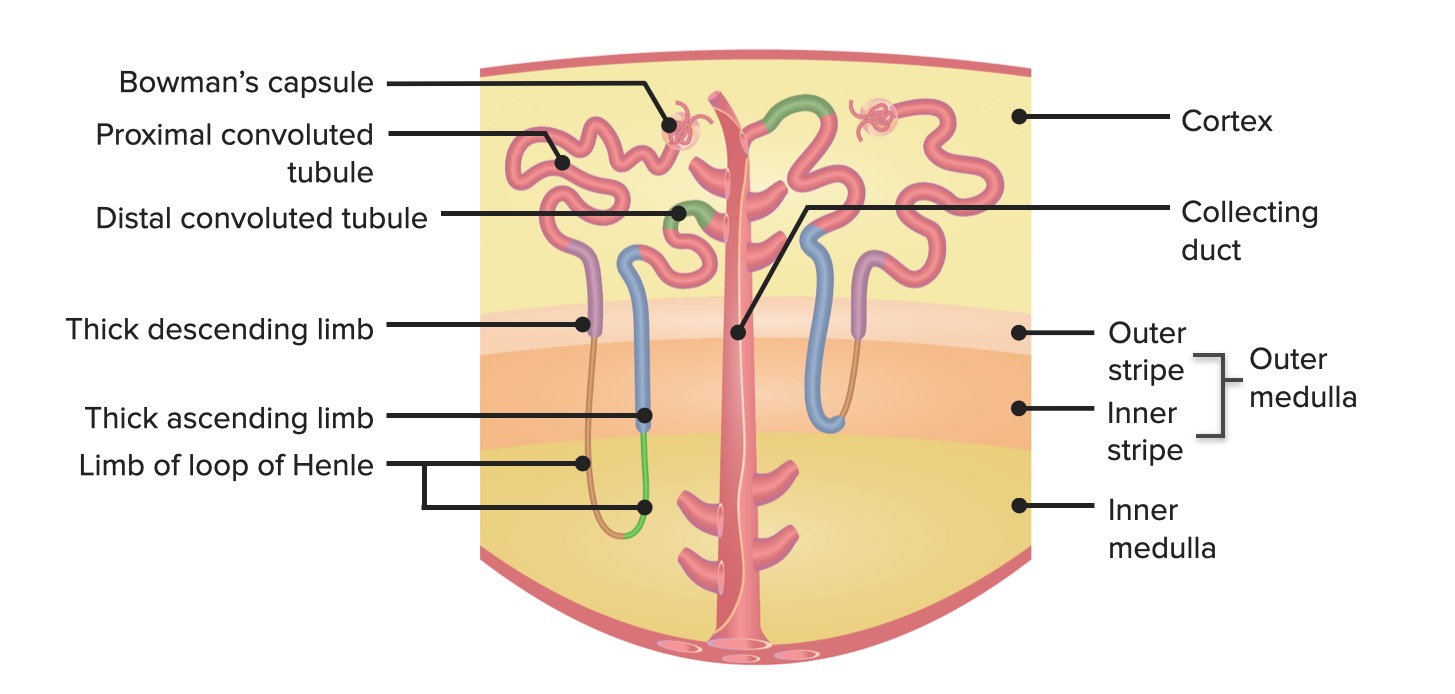
00:01 So when we think about the clinical manifestations of hypokalemia, they're actually multi targeted. 00:06 You can have cardiovascular manifestations and those are really the most serious. 00:11 So we might see cardiac arrhythmias and EKG abnormalities. 00:14 This includes premature atrial and ventricular beats. 00:17 Sinus bradycardia, atrioventricular block or ventricular, tachycardia and fibrillation. 00:24 We can also see signs on EKG. 00:26 We have a decrease in the amplitude of the T wave and an increase in the amplitude of the you U-wave which is shown here in this EKG. 00:32 We tend to see those primarily in the in the precordial leads. 00:37 We also have muscular manifestations from having hypokalemia. 00:41 So patients can feel weakness and muscle cramps. 00:44 A low potassium typically less than 2.5 million equivalents per liter can hyperpolarize skeletal muscle impairing contraction. 00:51 This can reduce skeletal muscle blood flow by empowering local nitric oxide release and predisposes to things like rhabdomyolysis breakdown of muscle during vigorous exercise. 01:01 Severe potassium depletion less than 2 milli equivalents can cause respiratory muscle weakness leading to respiratory failure and death. 01:07 So it's important to replete these patients when they present with such severe hypokalemia, and finally we can CGI muscle weakness as well which can result in Ileus bowel obstruction due to a decrease in muscular activity in coordination. 01:20 Now hypokalemia also has hormonal effects so it can impair insulin release and end-organ sensitivity to insulin. 01:27 So what that translates to is our patients can have worsened control if they're a diabetic, and I want you to think about that just for a second because patients who are on thiazide diuretics if they're hypokalemic then that can actually and they're diabetic that can translate into worsening glycemic control for those particular patients. 01:46 And then finally hypokalemia itself can have renal manifestation. 01:50 If somebody has prolonged hypokalemia, and we're talking usually years that can cause tubule interstitial and cystic changes in the parenchyma of the kidney. 01:59 So in patients who have chronic eating disorders, anorexia, bulimia, and they have chronic hypokalemia, they can often time manifest with hypokalemic nephropathy. 02:10 These patients often times are polyuric because they lose that concentrating ability because of where that hypokalemic nephropathy is and where those cystic changes happen that actually impairs the medullary gradient. 02:21 And again, they also have an increase in thirst and they develop this mild nephrogenic diabetes insipidus. 02:27 Hypokalemia itself can worsen hypertension. 02:30 This is important again in the patient population that we take care of. 02:33 It can increaserenal vascular resistance and it can also sensitive vessels to endogenous vasoconstrictors. 02:39 So a hypokalemic patient can worsen their hypertensive control. 02:43 Again, very important to recognize and then correct this.
About the Lecture
The lecture Hypokalemia: Clinical Manifestations by Amy Sussman, MD is from the course Potassium Disorders: Hypo- and Hyperkalemia.
Included Quiz Questions
Which of the following is associated with hypokalemia?
- Increase in the amplitude of the U wave on ECG
- Extended depolarization of the muscle endplate
- Increased end-organ insulin sensitivity
- Oliguria
- Increased resistance to endogenous vasoconstrictors
Author of lecture Hypokalemia: Clinical Manifestations

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excelent explication! I really like the explication because it has all the hiperkalemia trastorns explained perfectly!
