Playlist
Show Playlist
Hide Playlist
Hyperkalemia and Hypokalemia

-
Slides Fluids electrolytes Special Surgery.pdf
-
Download Lecture Overview
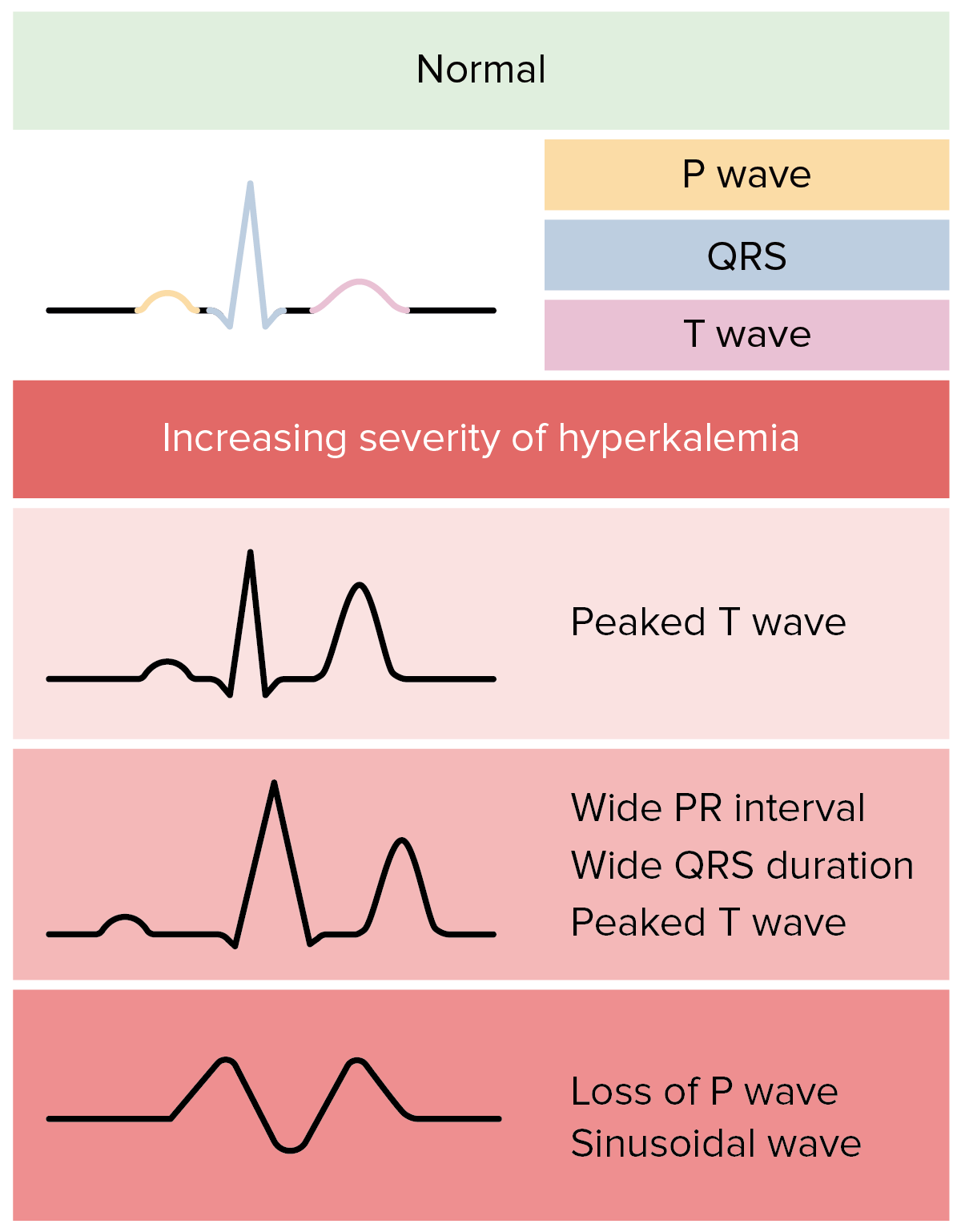
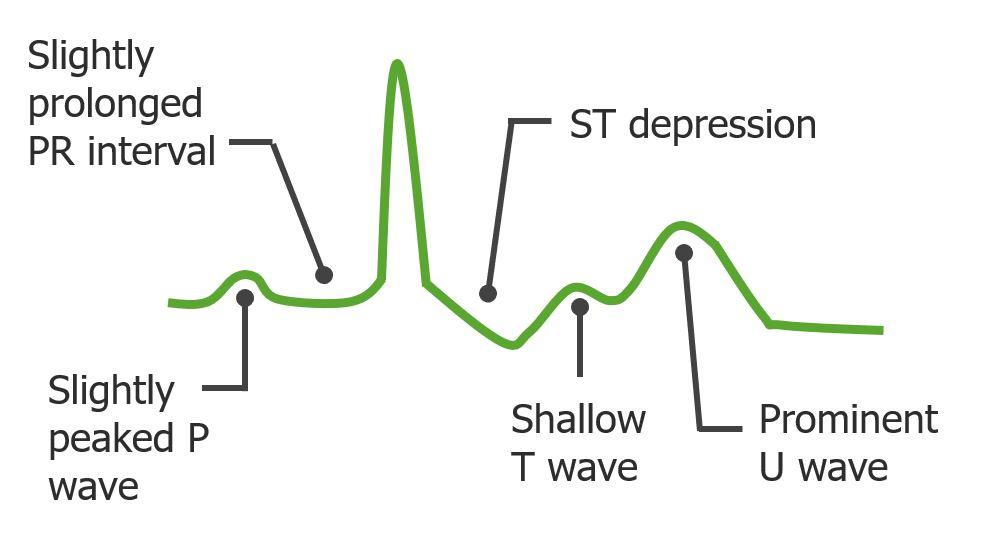
00:01 What happens when we have a lot of or an excess potassium, also known as hyperkalemia. 00:08 Hyperkalemia can reflect the removal of infusions, cellular breakdown such as tumor lysis or Rhabdo, trans-cellular shifting, which is actually very, very important and in this specific incidence in hyperkalemia, trans-cellular shifting is associated with acidemia. 00:30 There may be impaired renal excretion also contributing to hyperkalemia. 00:36 What are some clinical consequences? Classically, EKG changes. 00:41 Please commit this to memory. 00:43 EKG changes associated with hyperkalemia include shortened QT intervals, peaked T waves, widened QRS and potentially, can progress to ventricular fibrillation. 00:57 Please keep in mind, that the EKG changes depend on the concentration of potassium in your serum. 01:02 With a serum potassium of 5.5 to 6.5 you get tall peaked T-waves. 01:08 A serum potassium of 6.5 to 8 adds the loss of the P-wave. 01:13 And if your serum potassium rises above 8 you get a widened QRS-komplex with a tall T-wave. 01:19 There are priorities in the management of hyperkalemia. 01:23 Because of the extensive and severe consequences of hyperkalemia on the heart, the first step is to stabilize the myocardium. 01:33 Then redistribute the potassium. 01:36 And if necessary, excrete the excess. 01:39 Let's discuss the individual actions of how we can manage hyperkalemia. 01:45 First, calcium gluconate. 01:47 Calcium gluconate contributes to membrane stabilization of the myocardium, induced by hyperkalemia. 01:55 Next, use of bicarb. 01:57 Recall that acidemia causes trans-cellular shifting of intracellular potassium into the extracellular space. 02:05 Bicarb increases the pH and drives the trans-cellular shifting in the reverse process. 02:10 This also releases hydrogen from the cell in exchange for potassium. 02:16 Insulin. 02:17 Insulin is important. 02:19 It also - because it potentiates is a sodium potassium ATPase, allowing the maintenance of the normal trans-cellular gradient of mostly intracellular potassium and extracellular sodium. 02:34 Another option is the usage of ß2 Agonists. 02:37 They are stimulating the cellular uptake of potassium. 02:40 We can also use binders and exchangers. 02:42 An example of this is Kayexalate. 02:44 If all those mechanisms don't work, we can institute dialysis as a last solution. 02:51 Let's move on to a discussion of hypokalemia when the potassium is too low. 02:57 This can also be equally dangerous. 03:01 Hypokalemia may be a reflection of changes to the true inadequate intake or again trans-cellular shifting, except in this situation it’s due to alkalemia. 03:13 Lasix or loop diuretics often cause hypokalemia. 03:16 And overall weakness and overall muscle dysfunction can also cause hypokalemia. 03:23 What are the EKG changes? I also recommend you commit this to memory. 03:28 Prolonged QT intervals. 03:31 U waves. 03:32 ST depression. 03:34 Depressed T waves, which is different than hyperkalemia where we see peaked T waves. 03:40 And ultimately, it can cause torsades if coupled with hypomagnesium. 03:45 How do we fix hypokalemia? Well, it’s simple. 03:51 Give more. 03:52 Now, an important clinical pearl. 03:54 Sometimes, on the wards, you continue repleting the potassium and yet your plasma potassium levels never actually come up. 04:01 Part of the reason this is happening is because as you’re repleting the plasma potassium it is actually shifting intracellularly. 04:08 This suggests to you that there's been far more depletion of potassium than you first recognized. 04:15 This is an incredibly high yield slide. 04:19 Let’s spend a little time here. 04:21 Electrolyte disturbances, again, are not only important for physiologic daily function, but incredibly high yield test topics. 04:29 In hyponatremia, the manifestations is one that do not correct too quickly because if one corrects more than 12 meq/L in 24-hour period, it can lead to osmotic demyelination syndrome. 04:43 It was formerly known as CPM. 04:46 The first line treatment for the syndrome of inappropriate secretion of ADH is fluid restriction. 04:52 Severe symptomatic cases may include the use of ADH antagonist such as Tolvaptan or Conivaptan. 05:01 Next, hypermagnesium. 05:05 Hypermagnesium decreases your deep tendon reflexes. 05:08 Remember those OB patients. 05:10 OB patients oftentimes get infusions of magnesium. 05:14 Now, one of the signs that they have too much magnesium is decreased deep tendon reflexes. 05:19 Next, hypocalcemia. 05:21 Hypocalcemia causes prolonged QT intervals and numbness around the mouth, potentially Tetany if extreme. 05:31 Hypocalcemia is an important concept discussed in the parathyroid lectures. 05:37 And lastly, hypercalcemia. 05:39 Hypercalcemia associated with hyperparathyroidism is associated with bony pain, renal failure and neurological disturbances. 05:49 This slide should be committed to memory to help you answer standardized examination questions. 05:54 Thank you very much for joining me on this discussion of fluids and electrolytes.
About the Lecture
The lecture Hyperkalemia and Hypokalemia by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Hyperkalemia is associated with which of the given EKG changes?
- Shortened QT
- Elevated ST segment
- Broad T waves
- Narrow PR interval
- Increased R wave amplitude
Which of the following EKG changes is NOT associated with hypokalemia?
- ST elevation
- ST depression
- Peaked P waves
- Prolonged QT interval
- U wave
Author of lecture Hyperkalemia and Hypokalemia

Kevin Pei, MD
Customer reviews
2,7 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
1 |
less interesting sfdg sdf fasd asf asf afsd afsd fasd fdas
very superficial ............................................................................... not informative, or organized .. although it is very important vital topic
clear and confident knows his stuff. hope he lectures more.
