Playlist
Show Playlist
Hide Playlist
Hodgkin Lymphoma – Lymphoma

-
Slides Lymphoma.pdf
-
Reference List Hematology.pdf
-
Download Lecture Overview
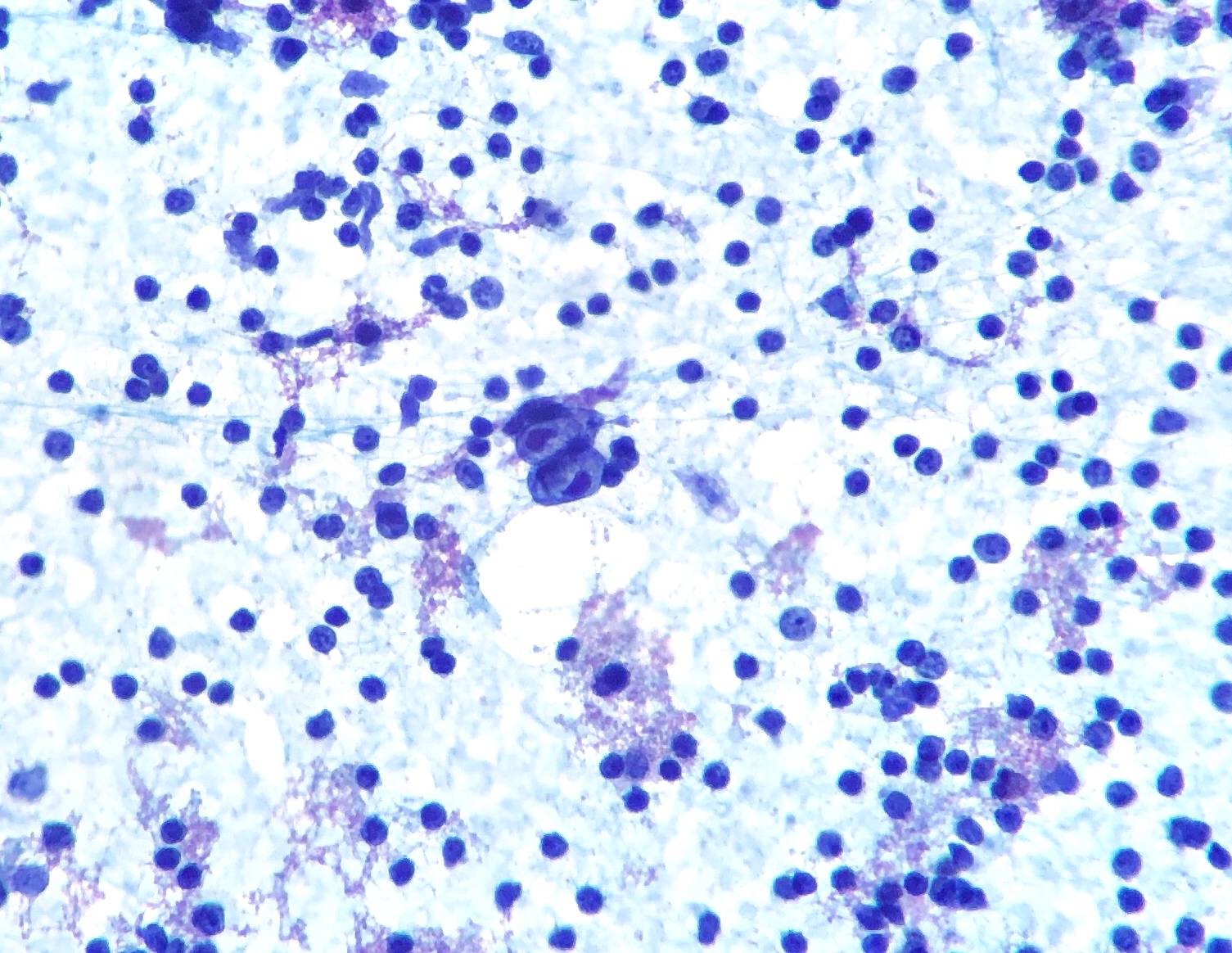
00:01 Hello. 00:02 Welcome to this lecture on the important topic of lymphoma. 00:06 In this lecture, you will learn a number of important points. 00:11 In lymphoma, the malignant lymphoid cells accumulate in lymphoid tissue rather than blood. 00:18 There are two broad subtypes of lymphoma. 00:22 Hodgkin lymphoma and non-Hodgkin lymphoma. 00:26 Hodgkin lymphoma is diagnosed by the presence of the Reed-Sternberg cell. 00:31 Whereas non Hodgkin’s lymphomas are an extremely heterogeneous group of disorders. 00:37 Now lymphoma is a disorder of malignant lymphoid cells. 00:45 But in lymphoma, these cells accumulate in lymphoid tissue, whereas in leukemia, they are mainly in the bone marrow and blood. 00:54 If we look at the slide on the right, you’ll see that this patient has a very large lymph node mass in the neck. 01:02 The incidents of lymphoma is increasing particularly non Hodgkin lymphoma. 01:08 We really don’t know the epidemiology behind this trend. 01:11 The treatment of lymphoma depends on the accurate diagnosis of the disease subtype. 01:18 And during this lecture we'll spend time working out how to make the correct diagnosis. 01:24 Let’s start with Hodgkin lymphoma. 01:29 This disorder which described by Thomas Hodgkin in 1832. 01:34 He worked at Guy’s Hospital in London. 01:38 And on the right, this very beautiful drawing, shows the original description of Hodgkin lymphoma from that time. 01:48 And it actually shows one of the major features of Hodgkin lymphoma which is it tends to spread down the lymphatic system, in this case from the neck into the axillary lymph nodes. 02:01 The most common presentation of Hodgkin lymphoma is with enlarged lymph nodes usually in the neck. 02:08 And as I said from the picture, it tends to spread through the lymphatic system rather than through other tissues. 02:16 There may be additional symptoms which are important in staging Hodgkin lymphoma. 02:22 These are fatigue, weight loss, and fever. 02:27 Now, the diagnosis of Hodgkin lymphoma, as with all diseases depends on the history, examination, and investigations. 02:38 On the history, should focus on the time course of the swelling of the lymph nodes which may indicate any other systemic symptoms as well. 02:49 EBV infection is an implicated as cause of many cases of Hodgkin lymphoma. 02:56 This is seen because there is evidence of EBV infection in many of the tumor cases. 03:02 And also, interestingly, when some people get their first EBV infection, they can get glandular fever or infectious mononucleosis. 03:12 Although that always clears up, many years later they do carry a high risk of developing Hodgkin lymphoma. 03:20 The examination of the patient should be of the major lymph node groups. 03:25 In the neck, under the arms, and in the abdomen and groin. 03:30 Blood test may show anemia and very often patient will have a CT or an MRI scan to look for evidence of disease. 03:42 On the right, you can see a chest x-ray showing mediastinal lymphadenopathy. 03:48 But to make the diagnosis you need to get some lymph node tissue and that biopsy is critical for looking for the Reed-Sternberg cell. 03:58 This is the characteristic feature of Hodgkin lymphoma, the Reed-Sternberg cell. 04:07 It’s an unusual cell in histology. 04:10 It is large, generally has a bilobed nucleus and has a very prominent nucleoli. 04:18 You can see some of the cells on that specimen which have a white cytoplasmic halo and a very prominent nucleolus. 04:27 The Reed-Sternberg cell is derived from a B cell and it’s expresses its mark such as CD15 and CD30. 04:37 And pathologists use these stains to make the diagnosis of Hodgkin lymphoma. 04:43 Pathologists also categorize Hodgkin lymphoma into 4 major types. 04:51 Nodular sclerosing, mixed cellularity, lymphocyte depleted, and lymphocyte predominant. 04:59 And this will affect the outlook and prognosis of the patient in some cases. 05:05 Now when a patient is diagnosed with Hodgkin lymphoma it’s very important to stage the disease. 05:12 And essentially what we’re doing here is seeing how far the disease has progressed because that will indicate the type of treatment that we need to give. 05:22 Hodgkin lymphoma is staged from I to IV. 05:28 Let’s look at this in more detail. 05:31 In stage I disease, there is swelling of a lymph node area in one region perhaps in the neck as shown on this picture. 05:41 In stage II, there is involvement of two lymph node groups but on the same side of the diaphragm, as you’ll see in the picture there, in which case we have lymph node swelling and mediastinal swelling. 05:57 Stage III disease, shows disease of above and below the diaphragm. 06:04 Whereas stage IV, is disseminated disease and involves non-lymphoid tissues perhaps the spleen or the bone marrow. 06:15 In addition, we also have to stage the disorder on whether the patients have systemic symptoms such as fevers or weight loss. 06:27 A, indicates the absence of these whereas B, indicates that these are present and that represents a more challenging disease to treat. 06:38 So a patient may be categorized as stage IIA or IIIB for example. 06:45 Now the treatment of Hodgkin lymphoma depends on the use of chemotherapy and radiotherapy in various degrees of combination. 06:57 The standard chemotherapy regimen for many years has been that ABVD regimen. 07:06 adriamycin, bleomycin, vinblastine, and dacarbazine. 07:12 And it’s a very effective treatment to Hodgkin Lymphoma. 07:16 Now one of the big questions when you are thinking about treatment of Hodgkin Lymphoma is the amount of chemotherapy and perhaps radiotherapy which you might want to give to the patient. 07:29 And doctors are moving towards trying to minimize the amount of treatment that is given so as to maintain a high cure rate while it’s limiting the side effects of chemotherapy and radiotherapy. 07:43 Here I’ve shown some examples of regimens that you might consider for different stages of disease. 07:50 So stage IA is very early disease, limited to one area and with no systemic symptoms. 07:57 And here, relatively short courses of chemotherapy or chemotherapy with small amounts of radiotherapy may be used. 08:05 For stage IB or II, you might want to give 4 to 6 courses of ABVD every month. 08:12 And maybe, only give radiotherapy to very large lymph node groups. 08:17 Whereas for more advanced disease you may wish to give a lot many more courses, 6 to 8 courses of ABVD and with radiotherapy to lymph nodes that remain at the end of treatment. 08:30 But people are always trying to improve and advance treatment and some centers use slightly different chemotherapy regimens, and there’s an example there of one that is used for intensive— for more intensive chemotherapy called BEACOPP which incorporates some additional chemotherapy agents. 08:50 Now the PET scan, the positron emission tomography scan is highly important in the treatment of Hodgkin lymphoma. 09:00 The PET scan involves the injection of fluorodeoxyglucose which is an analogue of glucose. 09:08 And it’s taken up by tumor cells, in this case Hodgkin lymphoma cells and then admits gamma rays. 09:16 These are detected by an external scanner, and it can be combined with the CT scan as a PETCT scan. 09:24 You can see that on the right. 09:27 Now PET scans are very useful for indicating areas of active tumor. 09:33 They can be useful for guiding the need for further treatment and also for distinguishing between tumor and scar tissue. 09:42 That’s particularly important in Hodgkin Lymphoma, because lymph nodes can remain large even after treatment when there is no active disease. 09:52 And the other area where PET scans are quite interesting is that they may be used to guide and potentially limit the amount of treatment that are given to individual patients. 10:03 So to titrate a therapy against the response. 10:08 The outcome for patients with Hodgkin Lymphoma are very good, Unfortunately relapse can occur, and this tends to be treated by different course of chemotherapy, a stem cell transplant, perhaps, using stem cells from the patient’s themselves called an autologous transplant or allogeneic transplant from another person. 10:34 Antibodies to block PD-L1 are emerging as a very effective immune therapy for Hodgkin lymphoma. 10:41 It may actually come to be used in first line therapy in future years. 10:46 And antibodies against CD30 which we learned early on as expressed on those Reed-Sternberg cells are also proving effective. 10:55 If we put all of these together, we can see that overall survival is excellent for patients with Hodgkin Lymphoma and over 85% of patients can achieve a long-term cure. 11:07 But the major concern with therapy in Hodgkin lymphoma is to avoid the complications of the treatment itself. 11:16 This could be seen as secondary malignancies many years later or cardiac toxicity from the chemotherapy and radiotherapy. 11:26 And that has driven the move to limit the chemo and radiotherapy to just a minimum needed for disease control.
About the Lecture
The lecture Hodgkin Lymphoma – Lymphoma by Paul Moss, PhD, OBE, FMed, FRCPath is from the course Hematologic Disorders.
Included Quiz Questions
Which of the following statements regarding the Reed-Sternberg cell is NOT true?
- It expresses CD8
- It is derived from a B cell
- It has very prominent nucleoli
- Its presence is diagnostic of Hodgkin lymphoma
- It expresses CD15
Which of the following statements is TRUE regarding the staging of lymphoma?
- Stage III involves lymph nodes affected both above and below the diaphragm.
- Stage IA indicates one group of lymph nodes involved and the presence of systemic symptoms (fever, night sweats, weight loss)
- Stage IB indicates one group of lymph nodes involved and the absence of systemic symptoms (fever, night sweats, weight loss)
- Stage II is characterized by involvement of the spleen
- Stage III is defined by the involvement of extralymphatic organs such as the bone marrow or liver.
Which of the following viruses is implicated in a subset of cases of Hodgkin lymphoma?
- Epstein-Barr virus (EBV)
- Human papillomavirus (HPV)
- Coronavirus
- Herpes simplex virus-2
- Hepatitis B
Which of the following is required to make a definitive diagnosis of Hodgkin lymphoma?
- Biopsy of affected tissue
- CT scan
- MRI
- Ultrasound
- Serology testing
Which of the following cell types gives rise to the Reed-Sternberg cell?
- B cells
- T cells
- Plasma cells
- Basophils
- Eosinophils
What are PET scans used for in patients with Hodgkin lymphoma?
- To guide the need for further treatment
- To determine the cause of the lymphoma
- To determine which chemotherapy agents will work best
- To determine if there is pulmonary toxicity from chemotherapy
- To diagnose lymphoma without the need for tissue biopsy
Author of lecture Hodgkin Lymphoma – Lymphoma

Paul Moss, PhD, OBE, FMed, FRCPath
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very easy, straight up to the point and very helpful
