Playlist
Show Playlist
Hide Playlist
Hereditary Hemochromatosis

-
Slides GD liver disease.pdf
-
Download Lecture Overview
00:01 Autosomal recessive, increase intestine iron absorption is the pathogenesis for hereditary hemochromatosis as we shall see. 00:09 Affects middle age men with the bronzing, and what that basically means is that this individual, take a look at your patient and you say, “My, goodness! You spent a lot of time in the tanning salon, didn’t you?” “Actually doc, I never did. 00:26 I actually never come out of my room because I had this amazing Play Station. 00:31 And so therefore if you never come out of the room but you look bronzed and there's a history in which you started seeing damage to your liver, oh, boy, you see hyperglycemia, there's no history of transfusion ever in this patient, you're thinking about hereditary hemochromatosis. 00:54 We talked about this in hematology as well where our topics there included HFE, hereditary, Fe, iron, and then also our topic with hepcidin and ferroportin. 01:08 Big time for your boards the understanding of this disease is showing up on your boards. 01:14 We’ll talk further about hemochromatosis and I’ll walk you through real quick once again, hereditary and primary. 01:23 Let’s continue. 01:24 Under hereditary liver disease, well, to say that it’s being caused by hemochromatosis. 01:31 Here you expect to find high ferritin iron saturation with iron overload. 01:36 We've talked about this in hematology hence I'm not going to great detail. 01:39 Close your eyes, let me walk you through this. 01:42 You're reabsorbing quite a bit of iron from your intestine, if you remember correctly the hepcidin levels will be low, therefore there's nothing stopping you or nothing stopping reabsorption of the iron from the intestine. 01:54 There's increase activity of ferroportin which is then bringing all this iron from the intestine into circulation. 02:01 Welcome to hereditary hemochromatosis. 02:04 Now, you give me the lab tests that you're going to find. 02:07 Ready? Iron studies. What's the first thing that you're gonna do? Remember? Serum iron obviously elevated. 02:16 Once iron comes out in the serum where is it going to store? Ferritin that will be high. 02:23 What’s the third thing that you're going to look for? TIBC. 02:27 If your ferritin levels are high, your TIBC will be low. 02:31 And tell me about saturation? Good, increased iron saturation. 02:38 If you're unclear about what we just did with iron studies, I highly recommend, you go back to hematology, obviously pathology and you take a look at our iron studies in great detail. 02:50 Now you need to start putting things together. This is an example of that. 02:54 Genetic testing. 02:58 You do wanna know about C282Y, remember how it’s done? and something that we talked about early with HFE. 03:06 If there's anything that you wanna take out of this at this point that is tested, is the C282Y. 03:12 If you're gonna remember H63D that’s on your own, but C282Y becomes important. 03:17 Let’s take a look at the management of hereditary hemochromatosis. 03:23 Keep in mind that this is hereditary. What was the name of the mutation that took place? It was the HFE gene, remember you can use those letters to your advantage, hereditary Fe. 03:35 What was the name of the particular protein, C282Y chromosome 6 in HLA-A3. 03:46 That would be increase absorption of iron from the intestine. 03:50 Management here, weekly phlebotomy until ferritin levels come down to approximately 50 mcg per liter. 03:58 Iron chelation therapy as well. 04:00 Now phlebotomy doesn’t reverse the cirrhosis, hypogonadism, or arthropathy, the triad that may take place with hereditary hemochromatosis. 04:07 Liver transplantation for advanced disease. 04:11 Remember with this, the iron could cause a damage to multiple organs, in fact they may result in restrictive cardiomyopathy, may knock at the pituitary, when it does then may result in secondary hypogonadism. 04:25 There's a high risk of hepatocytic carcinoma, so therefore annual screening is required. 04:31 And first degree relative should also be screened cuz you're worried about obviously inheritance patterns.
About the Lecture
The lecture Hereditary Hemochromatosis by Carlo Raj, MD is from the course Liver Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following signs is NOT related to hereditary hemochromatosis?
- Kayser-Fleischer ring
- Hepatomegaly
- Bronze-colored skin
- Hypogonadism
- Arthropathy
Which of the following statements regarding hemochromatosis is TRUE?
- Hepcidin levels are low.
- Iron saturation is low.
- Ferritin levels are low.
- Ferroportin activity is low.
- Serum iron is low.
Which of the following represents best the iron panel of a patient with hemochromatosis?
- Serum iron — high Ferritin — high Total iron-binding capacity — low Transferrin saturation — high
- Serum iron — low Ferritin — low Total iron-binding capacity — low Transferrin saturation — high
- Serum iron — high Ferritin — low Total iron-binding capacity — low Transferrin saturation — high
- Serum iron — high Ferritin — low Total iron-binding capacity — high Transferrin saturation — high
- Serum iron — high Ferritin — low Total iron-binding capacity — high Transferrin saturation — low
Which of the following is the MOST common chromosome involved in mutations of the HFE gene?
- Chromosome 6
- Chromosome 8
- Chromosome 12
- Chromosome 20
- Chromosome 3
Which cardiac manifestation does NOT occur in a patient with hereditary hemochromatosis?
- Vegetations on the heart valves
- Dilated cardiomyopathy
- Restrictive cardiomyopathy
- Congestive heart failure
- Arrhythmia
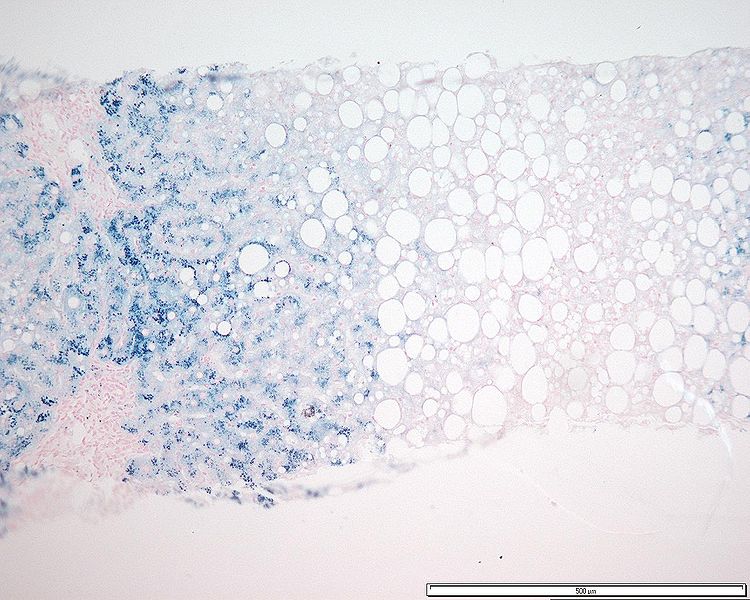
What is the color of iron in a slide of a liver biopsy taken from a patient with hemochromatosis?
- Brown
- Black
- Eosin
- Dark purple
- Greenish-brown
Author of lecture Hereditary Hemochromatosis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
