Playlist
Show Playlist
Hide Playlist
Hepatitis C Virus (HCV) – Flaviviruses

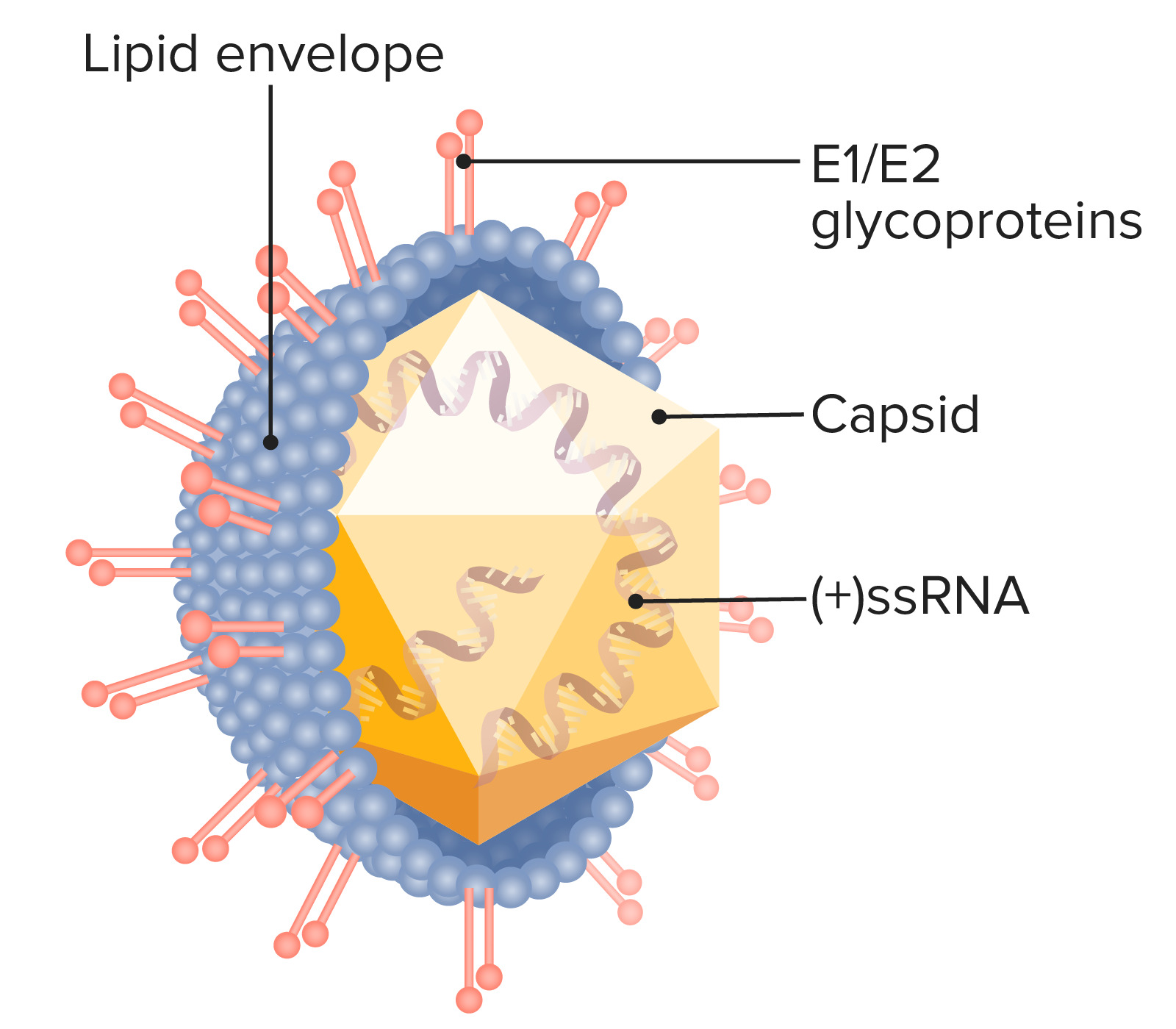
00:01 So let's start with hepatitis C virus. 00:04 Transmitted via a parenteral or blood exposure route, but also exposure to other blood and body fluids, via sexual contact or perinatal exposure - a baby's born to hepatitis C-infected mothers. 00:17 The clinical manifestations are, or include acute infection, which overall, is milder than hepatitis B virus, a chronic infection which occurs in 3/4 of the cases. 00:30 The viremia associated with that chronic infection lasts for at least, in fact, frequently over 10 years, and occasionally not as severely as hepatitis B but occasionally is associated with progression to cirrhosis of the liver with liver failure and a need for transplantation. 00:49 Antibodies acquired during any stage of this don't give immunity, and in fact, it has been difficult to obtain and create, I should say, a successful hepatitis C vaccine because the envelope proteins expressed by hepatitis C are quite variable there's changing, so it's a shifting target. 01:09 Looking at the table on the right side of the slide, is a bit of a closer drill down to what acute hepatitis looks like in the setting of hepatitis C. 01:19 The prodromal phase is very much a non-specific, viral illness with fever, malaise, and anorexia. 01:27 The preicteric, meaning prior to onset of jaundice and liver failure, is an escalation of gastrointestinal- type symptoms, so nausea, vomiting, nonspecific abdominal pain, and then fever with rigors. 01:41 And then the icteric phase when there is an acute hepatitis, assuming that the patient hasn't bypassed that and gone into the chronic phase. 01:50 But acutely, there will be rapid onset of jaundice with dark urine, increasing liver enzymes, exactly as you would expect, and even a mild hepatitis A case where there's acute hepatitis. 02:02 The CDC recommends hepatitis C screening for 2 populations. 02:07 First, all adults over the age of 18 should be tested once in their lifetime. 02:12 And second, all pregnant women during each pregnancy should be tested once. 02:16 The exception to these rules is in areas where the prevalence of HCV infections is below point 0.1%. 02:23 The universal screening is performed in a stepwise approach. 02:26 The first test performed to look for the presence of HCV antibodies. 02:30 Positive reaction. 02:31 This test means the patient's immune system has either been exposed to the virus at a previous point in time or there's an active infection. 02:38 This test alone doesn't discriminate between these two possibilities. 02:42 So if positive, a second test is done looking for HCV RNA. 02:46 If there's positive reaction in this test, the patient is determined to have an active viral infection. 02:54 The flowchart in this slide represents the testing protocol for working with a patient who is suspected of having an HCV infection. 03:00 Notice that unlike in the universal screening protocol, testing for the HV antibodies, as well as the HCV RNA are done simultaneously, rather than in a stepwise approach. 03:11 This change is made as a way to prevent false negative results for patients who may have been recently exposed to the virus, but not had enough time to mount a sufficient immunological response to form antibodies. 03:25 Here we can see a chart that plots antibody levels over time. 03:29 This red box in the lower left corner illustrates the window I mentioned on the previous slide. 03:34 This is effectively the lag and time between a virus exposure in the immune systems response to generate antibodies to the detectable level. 03:42 As you can see, this immune system response can take up to 2 months, during which time a test looking only for HCV antibodies would be negative. 03:50 During this window, liver enzymes can begin to rise. 03:53 So a new hepatitis workup should include both an HCV antibody test as well as a simultaneous test for HCV RNA. 04:01 If the HCV antibody test is negative, while the HCV RNA test is positive, that would indicate the patient has an acute HCV infection. 04:11 Prevention and treatment. 04:13 Well, of course, the best treatment is prevention, in the first place, and so all blood or blood donors and transplant for solid organ donors are screened by ELISA, which is a very sensitive way to look for presence of hepatitis C. 04:27 For those patients who become infected through a parenteral or sexually-acquired exposure, or even those babies born to a hepatitis C-infected mother. 04:37 Treatment for HCV is recommended for nearly all patients and typically consists of various combinations of four direct acting antiviral medications. 04:48 Each of these medications interferes with the specific HCV proliferation process. 04:54 With treatment patients can become permanently cured of the disease, with most experiencing a normalization of AST levels and cessation of histological progression of the liver disease. 05:05 Initial direct-acting antiviral regimens are no longer dependent on knowing the HCV genotype. However, obtaining HCV genotype testing may still be of benefit for future reference in the case of suspected treatment failure or repeat infection. 05:21 However, testing may not be readily available for some, and should not prevent initiation of therapy. 05:27 Treatment results tend to be more favorable in patients with less fibrosis in comparison with those with cirrhosis. 05:34 The medications are very expensive, but ultimately represent a cost-effective treatment when compared to the medical complications secondary to the incomplete treatment of this disease. 05:46 This slide depicts the typical proliferation cycle of HCV, which each of the 4 green boxes representing the target of an antiviral medication. 05:56 These include protease inhibitors, NS5A inhibitors, NNP inhibitors and NS5B polymerase inhibitors. 06:06 The combination of glecaprevir and pibrentasvir or ledipasvir and sofosbuvir are currently the antiviral regimens of choice for the majority of patients with chronic HCV infections in the United States.
About the Lecture
The lecture Hepatitis C Virus (HCV) – Flaviviruses by Sean Elliott, MD is from the course Viruses.
Included Quiz Questions
Which of the following corresponds with the approximate percentage of patients that will develop chronic infection as a clinical manifestation of hepatitis C virus?
- 75%
- 10%
- 25%
- 50%
- 85%
The investigation of choice for the screening of hepatitis C infection in blood or solid organ donors is...
- ...enzyme-linked immunosorbent assay (ELISA).
- ...recombinant immunoblot assay (RIBA).
- ...qualitative polymerase chain reaction (PCR).
- ...quantitative polymerase chain reaction (PCR).
- ... histological evaluation.
Author of lecture Hepatitis C Virus (HCV) – Flaviviruses

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
