Playlist
Show Playlist
Hide Playlist
Helicobacter Pylori

-
01-15 Helicobacter.pdf
-
Download Lecture Overview
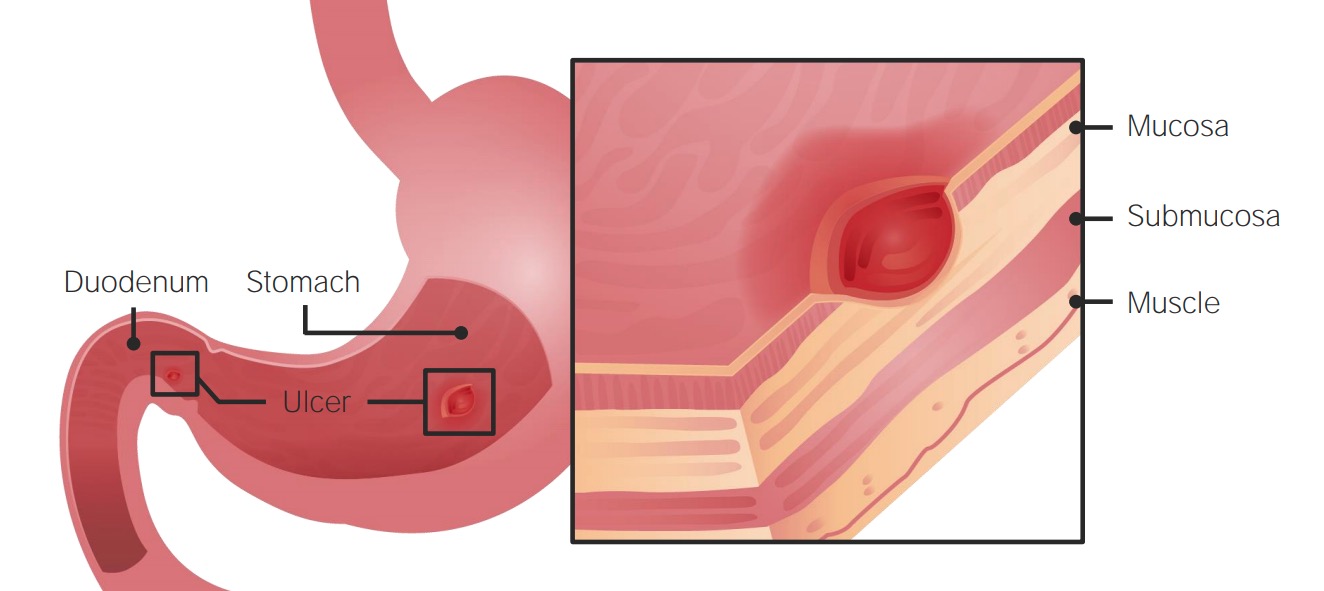
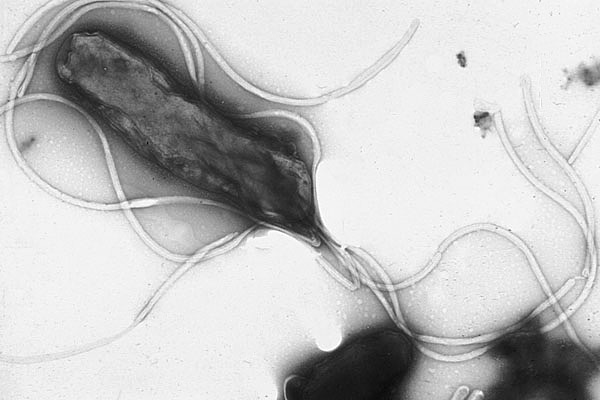
00:00 Most of us however, 50% are colonized by the time we reach age 65 years. 00:05 Helicobacter are gram-negative motile-rods which have a almost novel curved or helical shape with multiple flagella. 00:13 As we'll see in just a little bit when we discuss pathogenesis, this helical or screw like shape is essential to allow the organism to insert itself through the mucosal layer of its enteric target and attach to underlying enterocytes. 00:25 to insert itself through the mucosal layer and attach to underlying cells. 00:27 Helicobacter are microaerophilic and they have very complex growth requirements, but they are oxidase, catalase, and urease positive. 00:37 The image on the screen shows in a scanning electron microscopy picture, the organism itself and the surrounding flagella which are all important to help it enter into the junction of the enterocytes. 00:51 Now, Helicobacter pylori are ubiquitous organisms. They indeed do exist everywhere. 00:57 And as many people have come to realize, the older one gets, the more often one is colonized with these. 01:05 They exist by ingestion and are typically associated with poor sanitation, They exist by ingestion and are typically associated with poor sanitation, meaning water supply, poorly prepared foods, but there is also person-to-person contact which allows them to develop. 01:20 Once the initial aspiration or ingestion of the organism occurs, they will set up shop as you see in the images in the stomach. 01:29 Typically, in the antrum, but also perhaps a little bit further on closer to the duodenal junction. 01:36 And their typical target is the superficial gastric cells. 01:41 As mentioned before, the prevalence of infection in children is quite low even though, children do typically explore the world through their mouths. 01:50 However, as we age and expose ourselves to a variety of poor choices, either for our foods or sometimes by being exposed to poor sanitation, we as adults become more and more colonized. 02:04 And those who are older adults and older adults in countries where sanitation is not up to first world standards become even more colonized. 02:14 Most of us however, 50% are colonized by the time we reach age 65 years. 02:20 Helicobacter pylori releases urease as a way to neutralise stomach acid. 02:24 This causes that outer gastric mucin gel layer to liquefy, allowing the bacteria to swim through and attach to the underlying gastric alveolar cells. 02:34 So how does Helicobacter pylori produce its pathogenesis? First and most important, is the targeting of the gut, along with that, Helicobacter pylori is very acid sensitive. 02:49 So in a way, it creates its own neutral or even alcohol and pH-based environment. 02:55 It does this by production of urease -"Ase"- an enzyme which cleaves urea into ammonia and carbon dioxide. 03:04 Those byproducts are able to neutralize the normally acidic pH of the gut and allows the Helicobacter to colonize that superficial layer. 03:15 Then as mentioned, the multiple flagella and that helical or screw like shape allows the organism to burrow itself through the mucous barrier and into the top layer; the mucosal surface of the stomach. 03:31 When there, the local alkaline effect triggers release of gastrin secretion or gastric acid from other surrounding parts of the stomach in an attempt to return back to the fully acidic environment. 03:47 However, this production of gastrin and an acid in a way creates further erosion of the stomach creating peptic ulcer disease and then putting the patient at risk for gastric metaplasia which increase the risk for gastric cancer. 04:04 So all these are simply due to the Helicobacter trying to create its own perfect environment in which to nest or burrow into the stomach. 04:12 While there however, because it is still a pathogenic bacteria, the Helicobacter pylori also create mucinase, again an enzyme to cleave the mucous structures and also cytotoxins. 04:27 The development and production of the toxins especially will then recruit inflammatory cells to the site of the infection. 04:35 And due to almost an innocent bystander type attack, the attempt to kill the Helicobacter pylori actually takes out other healthy gut tissue furthering the damage of the peptic ulcer disease. 04:49 Helicobacter pylori is very common and is in fact the most common chronic bacterial infection in humans. 04:56 It can be identified in the gastric biopsy with the routine and stain as seen in the lower left part of the slide. 05:02 But there are also special stains that highlight the organism even better, including the worth in stari silver stains and gums stains as seen in the lower left with the hand stain. 05:13 Early acute superficial gastritis is caused by Helicobacter pylori. 05:18 You can see the marked neutrophil infiltrates as they appear in the mucosal neck region and lamina with the pit micro abscess as shown by that red arrow. 05:27 On the lower right is a Werth and star silver stain, which demonstrates easily many of the H. Pylori organisms colonizing the surface of regenerative gastric epithelium. 05:38 So how do we know all this? It's actually been very difficult to demonstrate because Helicobacter pylori is so ubiquitous. 05:46 The link between the organisms presence in the stomach and the development of gastritis or acid-based disease was more definitively demonstrated by Dr. Barry Marshall, one of two researchers; physicians who studied the link. 06:02 Dr. Marshall, very committed to his science and very committed to demonstrating the link drank a flask of active Helicobacter pylori and then charted the development in himself of peptic ulcer disease. 06:17 When neutralizing the acid, his disease started to improve. 06:20 So as close as was possible, using himself as a test subject, he demonstrated Koch's postulates and definitively demonstrated the link between the organism and gastritis. 06:31 Once that was demonstrated, it was then easier to demonstrate the secondary risks for gastric and duodenal ulcers. 06:39 And then the chronic atrophic gastritis further down putting patients at risk for known complications of gastric adenocarcinomas and the low-grade gastric malignant lymphoma's. 06:51 So without drinking our own flask of Helicobacter pylori, how can we demonstrate the presence of the organism present within ourselves as a risk factor for developing peptic ulcer disease? One mechanism is to use the Campylobacter like organism test; the CLO test. 07:10 Helicobacter pylori shares many cell wall components similar to Campylobacter and thus one can test for those components with an antibody reaction. Also, serologic tests exists. 07:24 Remembering again, that an immune reaction does occur to the Helicobacter pylori infection along with antibody production. 07:32 However, the most common mechanisms to demonstrate Helicobacter pylori are a radiolabeled urea breath test and a stool antigen test. 07:41 The stool antigen test; again, fluorescent antibody reaction against antigens expressed by the Helicobacter wall. 07:48 The radiolabeled urea breath test incorporates its presence of urease to demonstrate positivity. 07:55 The patient drinks radiolabeled carbon-14 urea and as the patient undergoes normal processing by the Helicobacter and urease, it delivers carbon dioxide and ammonia. 08:10 The ammonia stays, the carbon dioxide is exhaled and can be measured. 08:15 So if one exhales, you know, radiolabeled carbon from carbon dioxide, then the patient most likely has active Helicobacter pylori in their stomach. 08:27 So, once that has been demonstrated and the patient has either early onset or very active peptic ulcer disease and gastritis, what can one do? And there are multiple triple drug regimens that have been recommended. 08:40 Triple drug meaning that a single agent and a single focus of therapy is not sufficient. 08:47 One can't just neutralize the acid to improve. One also has to treat the organism. 08:53 So the first combination which you see here; combination of a bismuth containing product, along with metronidazole; an antibiotic to cover anaerobes, and either amoxicillin or tetracycline has partial success. 09:08 The similar combination of the bismuth salt with ranitidine and clarithromycin, also partial success. But the most definitively successful regimen is this one here. 09:19 Combining amoxicillin with clarithromycin and a proton pump inhibitor, something such as omeprazole. 09:27 However, this regimen needs to be conducted for more than several weeks along with modification of dietary regimen, rest, relaxation, the whole 9 yards. 09:38 So Helicobacter pylori is not our friend. 09:43 Unfortunately, it's quite ubiquitous and if one has it and unfortunately as one gets older, one likely does. 09:50 There is an increased risk for peptic ulcer disease, gastritis and the secondary complications of malignancies. 09:58 To avoid that, eat well and eat healthy.
About the Lecture
The lecture Helicobacter Pylori by Sean Elliott, MD is from the course Bacteria.
Included Quiz Questions
Which type of special stain can be used to highlight Helicobacter pylori under a light microscope?
- Silver stain
- Hematoxylin and eosin stain
- Gram stain
- Romanowsky stain
- Periodic acid-Schiff stain
Which structure of Helicobacter pylori allows it to attach to the superficial gastric cells?
- Flagella
- Cell wall
- Cell membrane
- Cilia
- Pseudopodia
Helicobacter pylori shares common features with which bacteria?
- Campylobacter jejuni
- Salmonella typhi
- Staphylococcus aureus
- Streptococcus pyogenes
- Proteus mirabilis
Which enzyme is produced by Helicobacter pylori to neutralize the acidic environment of the stomach?
- Urease
- Hydroxylase
- Oxidase
- Catalase
- Lipase
Which of the following is/are common non-invasive test(s) used to diagnose active Helicobacter pylori infection? Select all that apply.
- Urea breath test
- Campylobacter-like organism (CLO) test
- Antinuclear antibody test
- Stool antigen test
Author of lecture Helicobacter Pylori

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
