Playlist
Show Playlist
Hide Playlist
Glaucoma: Types

-
Slides Optic Pathology Glaucoma.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
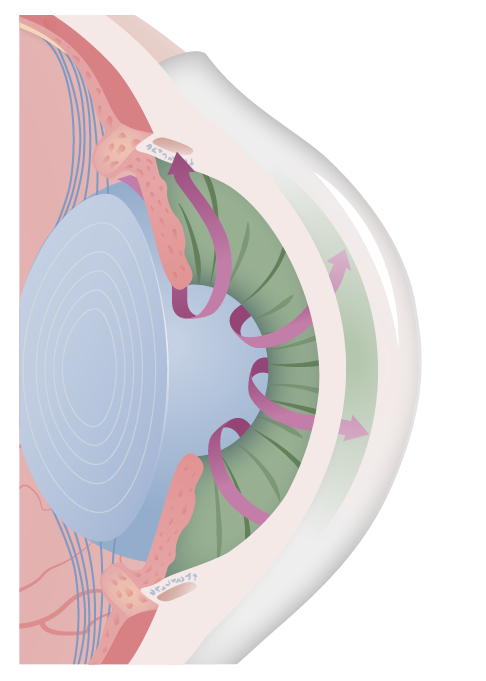
00:01 So, as promised, there are different forms of glaucoma there's a closed-angle glaucoma and open-angle glaucoma and a normal-pressure glaucoma. 00:11 Let's look first at closed-angle glaucoma. 00:14 This one is the easiest for me to visualize in my mind's eye about what's going on here. 00:20 So, up above is going to be our cornea, we're going to have the anterior chamber above the iris, we see the iris there. 00:28 And the iris is actually, there should be an opening that allows that green arrow to flow the fluid between the iris and the lens and out through the pupil into the anterior chamber where it can access the trabecular meshwork. 00:43 And where it can flow out through the canal of schlemm. 00:46 And what's going on here is that for various reasons, the lenses a budding onto the iris. 00:55 And now we can't get that flow out of there. 00:57 So it makes sense, it's called a closed-angle because we cannot flow fluid out, okay. 01:07 The aqueous humor outflow is blocked from the posterior chamber where it's being generated. 01:12 Remember the posterior chamber is that little bit behind the iris in front of the lens and we can't get it out to the anterior chamber. 01:22 Why can this happen? So we can have a very shallow anterior chamber. 01:27 Okay, if it just the configuration of the cornea, the lens and everything else that space gets squished. 01:34 The lens size can be big, you can have a much larger lens or distortion of lens that presses it up against the iris. 01:43 You can have it displaced. 01:44 So instead of being kind of posteriorly situated, it can be, float forward, if you will, and have a more anterior location and therefore a but on top of the iris. 01:58 And you can have a very narrow entrance to the anterior chamber angle. 02:02 So it just because of the way that the anatomy is assembled. 02:08 Secondary causes. 02:09 So if you get inflammation of the uvea, okay, so of the iris or of the ciliary body, then that clearly will cause some edema. 02:18 And that edema can expand those tissues where they previously would have flow. 02:23 Now there are edematous and they abut one another. 02:26 So uveitis will do that. 02:28 Trauma can clearly do this by causing damage, causing hemorrhage, causing a variety of other things that will also affect the general anatomy of that angle. 02:38 Steroids also influence blood flow, they also influence the anatomical kind of colocation of these various structures. 02:48 And then retinopathies, things that are actually impact the retina more posteriorly can have an impact on the geometry that's going on here. 02:59 So basically, in closed-angle glaucoma, it's a problem of geometry. 03:05 We're not able to get the normal flow from the ciliary body out from the posterior chamber into the pupil and out through the canal of schlemm and the trabecular meshwork. 03:18 Okay, it's basically the geometry. 03:22 And although it's very easy to understand, it's not the most common cause of glaucoma. 03:27 So closed or narrow angle glaucoma is only 20% of all glaucomas. 03:33 It tends to be more severe than open-angle glaucoma. 03:36 And this is kind of understandable because we've basically have blocked flow and we're continuing to crank out lots and lots of aqueous fluid. 03:44 It is associated with increased age, so just the vagaries of aging, we will have some changes in the geometry of the anterior and posterior chambers of the eye with all those various structures there. 03:56 Overall, due to the higher prevalence of open-angle glaucoma, glaucoma is more common in the African American ethnicity than it is in the Caucasian or Asian ethnicities. 04:07 However, closed-angle glaucoma is more common in patients of Asian and Inuit descent. 04:13 And they're very much can be a family history. 04:15 So if you think about it, you know, all these structures have a genetic basis for how they're organized and how they're put together, how they're assembled and how they lay relative to one another. 04:25 And if dad had a slight change in geometry, it's very possible that you might have a slight change in geometry. 04:31 So family history is very common. 04:34 Okay, that's closed-angle glaucoma, and if they say that's the one that's easiest for me to kind of understand. 04:40 Let's look at open-angle glaucoma. 04:41 In open-angle glaucoma in fact, the flow looks to be just fine. 04:47 The geometry is normal. 04:50 We have the ciliary body that's cranking out aqueous fluid. 04:54 It's able to get out between the iris and the lens. 04:58 It's able to get out through the pupil, it's able to move through into the trabecular meshwork Oh my goodness, everything looks fine. 05:06 So it's not, you know, it's not the geometry anymore. 05:10 So what else is going on here? Well, in fact it's the green box says at the bottom, you can have that trabecular meshwork, the canal of schlemm where the fluid is supposed to be going out, it can be blocked. 05:21 So basically now, this is a drainage problem. 05:24 This is not a geometry problem. 05:26 But there is now junk clogging the sewer drain, the canal, a schlemm, the trabecular meshwork, allowing fluid out that can be blocked from white cells or just inflammation in general. 05:39 So an uveitis, inflammation of the ciliary body and the iris or the choroid can actually cause now edema or increased white cells that can sit in the sewer grate and prevent the fluid from getting out. 05:53 If you have a vitreous hemorrhage, if you have a hemorrhage of any kind, red cells can get in there and kind of clog up the works. 05:59 And if you have a retinal detachment or you have a retinopathy, those elements can also float around and end up blocking the outflow. 06:08 So this is a clogged sewer drain is another way to think about open-angle glaucoma. 06:14 So there can be a couple different primary causes. 06:19 So it's not just that there's clogging, you can actually have a little over aggressive, a little, you know, a little too enthusiastic production of the aqueous humor by the ciliary body and there's more production than can be successfully drained. 06:34 Okay, that kind of makes sense or you can have decreased drainage. 06:38 Either one of those will lead now to increased fluid pressure within that anterior chamber which eventually then translocates and has effects on the optic nerve. 06:49 Secondary causes, so we can have as we talked about previously, blockage of the trabecular meshwork, clogging of the sewer drain with white cells from an uveitis, red cells from a vitreous hemorrhage or retinal detachment elements. 07:02 Okay, good. 07:04 This is the most common cause of glaucoma, open-angle glaucoma. 07:10 Like other forms of glaucoma, it is associated with increasing age. 07:14 So if you have more junk, and more junk over time that may block your fluid going out. 07:21 As I said before, glaucoma overall is more frequently seen in African American ethnicity. 07:30 But open-angle glaucoma is no exception. 07:33 And there may well be a family history. 07:34 So again, if mom has a chronic overproduction of aqueous fluid, then you may have an overproduction of aqueous fluid because of the same genetic variation. 07:48 And then there's normal pressure glaucoma. 07:51 This one is basically has all the same features of primary open-angle glaucoma, the entity we just described, fluid is flowing appropriately, everything's open, nothing's closed, and nothing is particularly blocked. 08:09 But you can still have optic nerve atrophy in the setting. 08:15 And the point about this is that it is probably still an effect of pressure. 08:23 But the pressures that we measure in the anterior chamber are within the normal limits. 08:29 So we haven't exceeded about that 21 mm Hg. 08:35 Why is this happening then since the pressure is not elevated? Well, in fact, there's probably more than just increased anterior chamber pressures that will be drivers for optic nerve atrophy and glaucoma. 08:47 And you can have subtle changes in vasculature that may compromise blood flow to the optic nerve and that may be a cause. 08:55 So... 08:57 if you're thinking about normal pressure glaucoma, it's the same as open-angle glaucoma in terms of the general anatomy, but the pressures are within the normal limits.
About the Lecture
The lecture Glaucoma: Types by Richard Mitchell, MD, PhD is from the course Diseases of the Anterior Chamber and Uvea.
Included Quiz Questions
What is the position of the lens in closed-angle glaucoma?
- The lens is located forward.
- The lens position is normal.
- The lens is located posteriorly.
- The lens is displaced sideward.
- The lens is displaced upward and forward.
What is an anatomic predisposition for closed-angle glaucoma?
- Shallow anterior chamber
- Color of the iris
- Size of the pupil
- Size of the palpebrae
- Curvature of the conjunctiva
Indiscriminate use of what drug can cause glaucoma?
- Steroids
- Antibiotics
- NSAIDs
- Retinoids
- Antimetabolites
What may block the canal of Schlemm, resulting in open-angle glaucoma?
- Retinal elements, WBCs, and RBCs
- Bacteria
- Platelets
- Fibrin
- Epithelial cells
What is the primary cause of open-angle glaucoma?
- Idiopathic overproduction of aqueous humor or decreased drainage of aqueous humor
- Blockage of the trabecular meshwork by RBCs
- Trauma to the uvea
- Retinopathy
What is the racial predilection for glaucoma?
- African American
- Hispanic
- Asian
- Caucasian
- Native American
Author of lecture Glaucoma: Types

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I appreciate your enthusiasm for this topic. Your lectures draw me in and I am able to understand the concepts you are discussing.
