Playlist
Show Playlist
Hide Playlist
Glaucoma: Introduction

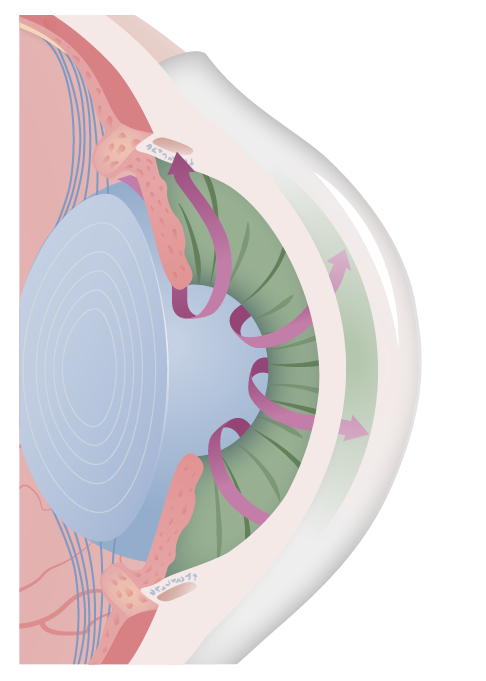
00:01 Our topic is glaucoma. 00:02 We are dividing glaucoma into open and close angle glaucoma. 00:06 In order for us to understand this, we must first understand the journey of the aqueous humor. 00:14 Remind me, where is aqueous humor being produced? Posterior chamber. 00:22 Can you picture where the posterior chamber is? Let's have a look. 00:26 So where am I? Make sure that you're clear about where we are. 00:31 On the left is the normal. 00:33 And what you're focusing here on the normal left picture on the far right will be the cornea. You see that? The bulge cornea. 00:44 The cornea, as you move in further obviously, you have the pupil, which is then formed by the iris, right? Now, what you wanna do next is that the iris then divides your chambers into interior and posterior chambers. 01:02 In another words, behind the iris is the posterior chamber, and then front of the iris would be the anterior chamber. 01:12 The production of your aqueous humor would be in the posterior chamber specifically in the ciliary body. 01:21 The drainage of your aqueous humor would have to be coming around your iris into the anterior chamber, and then 90% of your aqueous humor is being drained by whom? By the trabecular meshwork specifically the canal of Schlemm. 01:42 Another 10% or so might be the uveoscleral drainage. 01:47 Our focus would be in pathology here. 01:49 The canal of Schlemm and what we call the iridocorneal junction. 01:59 Now, what may then happen is that let's say that junction becomes closed? The angle. 02:07 Whenever we talk about closed angle and open angle, what angle are we all referring to as clinicians? The angle between the irido, the iris, and the cornea. 02:19 Are we good? In that particular junction we have the trabecular meshwork. 02:26 So now let's say that the angle closes. 02:30 You don't have drainage. You're gonna have increase intraocular pressure. 02:36 Or the trabecular meshwork may then become gummed up. 02:42 In other words idiopathically most common, African-American most common in terms of gender, race, and you will then have open-angle glaucoma. 02:54 That where our focus would be on? we have two chambers, posterior and anterior. 02:58 Now on the right, look at what has happened. 03:03 We have that angle which has now been closed. 03:05 So when that angle has been closed, look at the arrow there. 03:10 That arrow represents the aqueous humor those being produce by the posterior chamber by the ciliary body. 03:16 It has nowhere to go, because the angle has been closed. 03:20 So what's gonna happen to the pressure? Increased. 03:23 We call this closed-angle glaucoma. 03:25 And we're going to further detail. Let's have a look. 03:28 So closed-angle glaucoma refers to the fact that the angle that's normally responsible for allowing the aqueous fluid or humor to move from the posterior chamber into the anterior chamber do not take place. 03:41 That angle has been lost. May I ask you something? So if that angle, narrow angle, has not been closed, what would you like to do with that iris, so that you could open up that angle? Would you like the ciliary body to relax and the iris that then open up and cause mydriasis? No. Because that would then may make things worse, correct? So what you want to promote is parasympathetic contraction, pinpoint, so that the iris is pulled in causing miosis, opening up that angle. 04:20 Are we good? Not to worry. 04:23 I'll repeat that again, as we get into management. 04:26 So here we have closed-angle glaucoma. 04:28 Let's go through the steps in pathogenesis. 04:31 Increase pressure as you can imagine. 04:33 We have intraocular pressure. 04:36 Technically speaking with closed-angle, you do have acute and chronic. 04:39 Our focus in pathology will be acute, acute closed-angle glaucoma. 04:44 Why? Because that's your emergency. 04:46 That's your sudden cloudiness, that's one in which, oh, my goodness! If left untreated goes into blindness. 04:51 So usually drained by the duct. 04:54 Next, what may then happen is the thickening of the lens. 04:58 The canal of Schlemm is compressed and so therefore can no longer drain the fluid. 05:01 There is incredibly high pressure taking place in the optic disc. 05:05 So what do you think is gonna happen? Picture the optic disc for me. 05:09 Are we there? Okay. 05:11 What is in the middle of that optic disc? What do we say that was called? The cup, right? The cup. 05:17 So now if you have backing up of pressure into the let's say the optic disc, what's gonna happen to that cup? That's gonna get larger. 05:26 What do we call that clinically? Cupping. 05:29 Let's further talk about pathogenesis. 05:33 Let's talk about the acute first. 05:36 Take a look at that angle. 05:38 Abolished. 05:39 If it's acute, this is it. 05:42 Medical Emergency! I think I'll talk loud enough. 05:47 If I get any louder I will blow out your ear drums. 05:49 Not a good thing but definitely, exclamation. 05:55 We have narrowing of the angles. What are you trying to do? Are we gonna take our time and decrease the production of aqueous humor? Really? Do you think you have that kind of time? Of course not. What do you wanna do? Man, open up that angle. Okay. How do you open that angle? If you use an Alpha-1 Agonist, let's use epinephrine let's say, then whoa, they're gonna relax the ciliary body, the iris is then going to become relaxed and you'll have mydriasis which means that you made matters worst. You don't wanna do that. 06:27 You wanna take that iris and pull it, contract it, so that then you cause miosis. 06:32 Welcome to M3 cholinergic receptor, right? That's what you're focusing on. 06:40 Not to worry, I'll repeat that again in management. Second time I said that. 06:44 Signs and symptoms. 06:46 Severe pain, photophobia, blurry vision, the red eye, steamy cornea. 06:53 Steamy cornea, look for that description. 06:55 The pupil is fixed, nonreactive to light, intraocular pressure so high. 07:01 You've lost ability for accommodation, is that clear? And the light reflexes no longer a relevant point. 07:09 This is an emergency. Acute type. Our focus will be acute. 07:14 Chronic could be asymptomatic. 07:14 You could have a chronic type of closed-angle, but our focus here would be on acute. 07:21 Is that clear? Management. So what are we doing? We're trying to give a parasympathetic cholinergic, so that we're gonna bring about miosis. 07:28 So then we could have pinpoint pupils, so that we open up that angle as quickly as possible. 07:33 Welcome to pilocarpine. 07:35 In addition, it could be systemic carbonic anhydrase inhibitor, but that's only so that you can decrease, hopefully, the aqueous humor production as quickly as possible. 07:44 More importantly though it's an M3 cholinergic agonist. M3. 07:50 Laser surgery as well. 07:52 We're gonna compare acute closed-angle with open-angle. 07:59 Take a look at the blue area here again, this time the posterior chamber, are you there? The posterior chamber over to the left a little bit, the production of aqueous humor continuous. 08:10 No form of angle, open and well, that trabecular meshwork should have been draining, but it's not. Why? I don't know. Do you? In other words, most common cause, we don't really know. 08:27 It's idiopathic. But then you could also have material that's being formed that's causing gumming up as what we call it in pathology. 08:35 In which you're not able to drain, so it's chronic. 08:38 So now what do you think your issue or should I say, what do you wanna do in terms of steps in management? The angles are already open, so why in the world would you think about giving M3 agonist, right? Why would you wanna give pilocarpine? Makes no sense. 08:51 So what you're trying to do is trying to open up that angle further, So that? excuse me, what you're trying to do is trying to facilitate the drainage, that's a better description, right? In terms of management. 09:02 So we'll talk about that or maybe decrease the production. 09:06 Let's continue. 09:08 The decreased rate of the aqueous humor outflow into the canal of Schlemm. 09:14 Know the description proper. 09:17 That's by definition open-angle glaucoma. 09:20 You should be bilateral. Aching. 09:23 What was it in closed-angle? Acute, sudden steamy cloud, red injected eye. 09:29 Ouch! It hurts, Doc! I can't even see out of this eye! It hurts and I can't even look at the light. 09:34 Nothing. Photophobia. 09:37 That's acute closed-angle. 09:38 That hurts so much, it's achy. 09:40 Now, in both instances the cupping could be taking place. 09:44 What cupping mean though? The cup will be the center portion of the optic disc where you have transmission of your vessels and nerve. 09:52 The cupping may then become larger. 09:54 Night blindness is a possibility and the gradual loss, look for this, the gradual loss of peripheral vision that may lead into tunnel vision, and of course, if left untreated, definitely gonna lead into blindness, correct? Management here, first line of drug, what you're trying to do is decrease the rate of flow into the eye. 10:15 Beta-blockers such as timolol, beta blockers. 10:19 Secondly, we have prostaglandin F2 alpha 2 agonist. 10:24 And these are be the latanoprost. 10:27 So those that have the term, latanoprostenum, represents the PGF2 Alpha 2 agonist. 10:33 What does that do? That then allows, hopefully, for further drainage of the fluid through the trabecular meshwork. 10:41 And here, Alpha adrenergic agonist, that decrease the production. 10:46 Maybe pilocarpine and remember, acetazolamide, carbonic anhydrase inhibitor. 10:52 And once again you could decrease the amount of aqueous humor production.
About the Lecture
The lecture Glaucoma: Introduction by Carlo Raj, MD is from the course Glaucoma. It contains the following chapters:
- Introduction to Glaucoma
- Closed Angle Glaucoma
- Open Angle Glaucoma
Included Quiz Questions
Which of the following statements regarding closed angle glaucoma is NOT true?
- Acute closed angle glaucoma presents with painless blurring of vision.
- Increased pressure inside the eyeball occurs as a result of lack of drainage of aqueous humor.
- It can be caused by closure of the canal of Schlemm.
- Increased pressure inside the eye causes damage to the optic nerve.
- Acute blockage is an ophthalmic emergency.
Which of the following medications is NOT used in the treatment of acute closed angle glaucoma?
- Atropine
- Alpha 2 agonists
- Beta blocker
- Topical cholinergic
- Acetazolamide
What is the most common cause of open angle glaucoma in the United States?
- Idiopathic
- Bowing of the iris
- Cataracts
- Obstruction of canal of Schlemm
- Decreased aqueous production
What is the first line medical management of open angle glaucoma?
- Prostaglandins
- Alpha agonists
- Calcium channel blockers
- Carbonic anhydrase inhibitor
- M3 cholinergic agonist
Aqueous humor is secreted from which structure?
- Ciliary body
- Canal of Schlemm
- Lens
- Iris
- Iridocorneal junction
Author of lecture Glaucoma: Introduction

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
This video helps me tremendously in understanding the pathology of glaucoma and how to differentiate angle-closure and open angle glaucoma. Excellent job Dr Raj. Thanks for everything!
