Playlist
Show Playlist
Hide Playlist
Gestational Hypertension (PIH), Preeclampsia (Toxemia) and Eclampsia

-
Slides GestationalHypertension Obstetrics.pdf
-
Download Lecture Overview
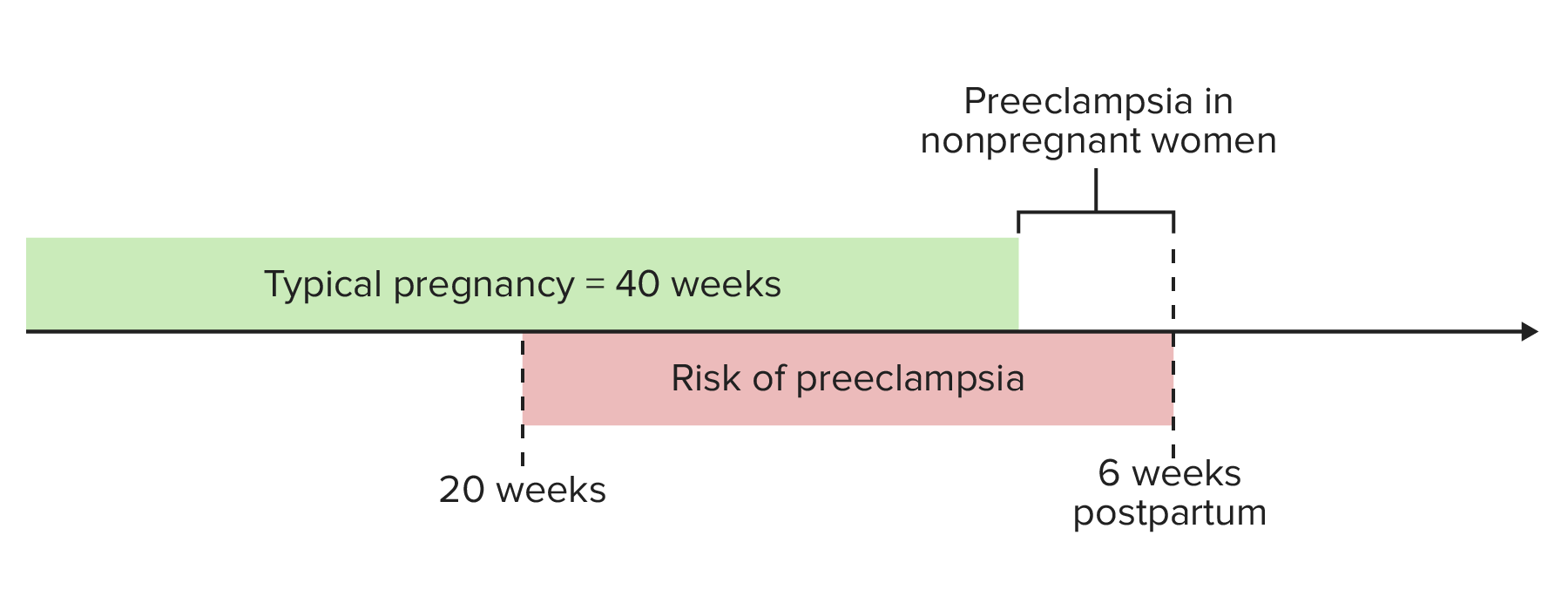
00:00 Now, let's discuss hypertensive disorders of pregnancy. There are 3 disorders that we need to discuss, and we'll start with gestational hypertension. So, gestational hypertension are blood pressures greater than 140/90, 2 blood pressure readings 6 hours apart, diagnosed after 20 weeks of gestation without proteinuria. If these blood pressures exist before 20 weeks, that's considered chronic hypertension. Moving on from gestational hypertension is preeclampsia. 00:35 Preeclampsia is hypertension with those same blood pressures that we just discussed with proteinuria. So that means protein in the urine. Let's look at preeclampsia in a little more detail. So these blood pressures again greater 140/90 but less than 160/110, a protein- creatinine ratio of 0.3, a 24-hour urine protein of greater than 300 mg, and absence of severe feature. All these features constitute preeclampsia with mild features. Now, preeclampsia can also be diagnosed with severe features. So, those are blood pressures greater than 160/110, new-onset cerebral or visual disturbances, these often manifest as an unrelenting headache or a headache not relieved by Tylenol, patients will often have visual disturbances such floaters, spots before their eyes. Any of those would give us the diagnosis of preeclampsia with severe features. Patients may also experience pulmonary edema. Also, a part of preeclampsia with severe features is something called HELLP syndrome. Again, this is another manifestation of preeclampsia with severe features, so you can have preeclampsia with severe features and not have HELLP syndrome. We're going to talk about HELLP syndrome in a little bit more detail. Also, if the patient has renal insufficiency, that gives them diagnosis of preeclampsia with severe features. A renal insufficiency is defined by a serum creatinine concentration greater than 1.1 mg/dL or a doubling of the serum creatinine concentration in the absence of other renal disease. 02:17 Pre-eclampsia with severe features is diagnosed when there is hypertension greater than a systolic of 160 or a diastolic of one to death alone, or when there is hypertension greater than a systolic of 140 and a diastolic over 90 proteinuria plus any other additional feature listed on this slide. 02:37 For instance, a blood pressure of 150 over 95 proteinuria and pulmonary edema would give us a diagnosis of pre-eclampsia with severe features. 02:48 So HELLP syndrome, that stands for hemolysis, elevated liver enzymes, and low platelets. Hemolysis is diagnosed by an elevated LDH. Elevated liver enzymes means an elevated AST and ALT, and low platelets are platelets less than 100,000. 03:10 Now, back to our hypertensive disorders of pregnancy. The 3rd and the most concerning is eclampsia. This is hypertension with proteinuria and also seizures. So, let's go through a case. 03:24 Maria is a 37-year-old gravida 1, para 0 female at 38 weeks' gestation that presents to triage with complaint of severe headache. She has no history of migraines or hypertension. On physical exam, her blood pressure is 180/110, her protein-creatinine ratio is 6. What is the next best step in her management? Would you say (A) immediately move to delivery via C-section, (B) immediately move to delivery via induction of labor, (C) start a labetalol IV infusion, or (D) start magnesium sulfate infusion? Let's go to the next slides to find that answer. So, when we're talking about our hypertensive disorders and how we treat them, let's start with gestational hypertension again. So, gestational hypertension is managed expectantly, meaning we don't start any antihypertensives and we deliver at 37 weeks. So let's talk about the treatment for preeclampsia. If it's preeclampsia with mild features, patient should be watched closely and we would expect to deliver at 37 weeks, but again let's go over what mild preeclampsia is. That's blood pressure greater than 140/90 but less than 160/110, a protein-creatinine ratio or PC ratio of 0.3, and a 24-hour urine protein of greater than 300 mg but less than 5 g. Now, preeclampsia with severe features, we're getting a little worse. So, with this we now need to give magnesium sulfate because we want to make sure these patients don't seize and they have an increased risk for that. We also want to give antihypertensive medications especially if our blood pressure starts to get greater than 160/110 which is part of the diagnosis of preeclampsia with severe features. We do want to control those blood pressures. Now, if the patient is over 34 weeks of gestation when she is diagnosed with preeclampsia with severe features, we would recommend delivery as this is the treatment for preeclampsia. So let's go through some of those treatments that we used in medications. So, first magnesium sulfate. We give this for seizure prophylaxis, not for antihypertension and not to lower the blood pressure, only to prevent seizures. The recommended dose is 4 or 6 g load with 2 g per hour, and we're not exactly sure how it works to stop seizures but we do know that it's a calcium channel blocker and this is the proposed method of how it works to actually stop seizures. Now, for our medications, alpha-methyldopa, labetalol, nifedipine, and hydralazine. One has not been proven to be better than another, and so it really is a matter of physician choice, clinical acumen as to which medication you start with, but you can see here they vary in doses and they vary in the amount that we give. All of them can be used for chronic hypertension, but only labetalol, nifedipine, and hydralazine are used in acute management. Moving on to eclampsia, now the main thing that we have to do for treatment of eclampsia is to stop the seizures. Before we do anything, we want to stabilize our patient and stop the seizures. Though delivery is cure, again we want to start that magnesium sulfate so that we can we stop those seizures. So let's go back to our patient, Maria. To recap, Maria is a 37-year-old gravida 1, para 0 female at 38 weeks' gestation that presents to triage with complaint of severe headache. She has no history of migraines or hypertension. On physical exam, her blood pressure is 180/110 and her protein-creatinine ratio is 6. What is the next best step in her management? What do you think? The answer is D. 07:18 We want to start magnesium sulfate. Remember the 1st thing we want to do is stabilize our patient and prevent seizures, and that's going to be magnesium sulfate. Well, let's talk about the other options. So immediately move to delivery via C-section or induction of labor. Well, the route of delivery, even though delivery is the cure for preeclampsia, the route of delivery depends on the mom. If the mom is remote from delivery, then we will say a C-section. 07:44 However, if the mom is stable and she has a favorable cervix, meaning her cervix is thin, dilated, it looks like she is favorable for a vaginal delivery, we can proceed with induction of labor. So, while delivery is the treatment for preeclampsia, we don't have to rush to deliver. 08:00 We always want to remember to stabilize our patient first.
About the Lecture
The lecture Gestational Hypertension (PIH), Preeclampsia (Toxemia) and Eclampsia by Veronica Gillispie, MD, MAS, FACOG is from the course Antenatal Care. It contains the following chapters:
- Hypertensive Disorders of Pregnancy
- Pre-eclampsia
- Eclampsia
- Treatment
Included Quiz Questions
A 34-year-old G4P3 woman presents for her 28-week antenatal check-up. She has no other past medical history. Her blood pressure is 145/100. She does not have glucosuria or proteinuria. If a repeat blood pressure is taken in 6 hours and is still above 140/90, what is the diagnosis?
- Gestational hypertension
- Chronic hypertension
- Preeclampsia
- Eclampsia
- None of the answer choices are correct
A 28-year-old G1P0 woman presents at 37 weeks gestation with new-onset swelling in her legs and hands, a 2-day history of headache that won't go away with rest and acetaminophen, and intermittent visual bright spots. On exam, she is found to have a blood pressure of 162/111, and a spot urine protein/creatinine ratio of 0.4. What is the most accurate diagnosis?
- Preeclampsia with severe features
- Preeclampsia without severe features
- Chronic hypertension
- Gestational hypertension
- Eclampsia
A 24-year-old G1P0 obese woman at 26 weeks gestation is seen for a routine prenatal visit. Her blood pressure is 158/100, her heart rate is normal, and her spot urine test is negative for glucose and protein. She denies any headaches, visual changes, chest pain, or difficulty breathing. A repeat blood pressure done 6 hrs later is 154/105. What is the most accurate diagnosis?
- Gestational hypertension
- Chronic hypertension
- Preeclampsia without severe features
- Eclampsia
- Preeclampsia with severe features
A 20-year-old female G1P0 with a twin pregnancy at 34 weeks gestational age presents to triage with one day of severe headache. Her blood pressure is 165/110 and her heart rate is 99. Her spot urine protein/creatinine ratio is 1. Her lactate dehydrogenase level is elevated, liver enzymes are elevated, and her platelets are 93,000. What are the diagnosis and next best step in management?
- Preeclampsia with HELLP syndrome, start magnesium sulfate and anti-hypertensives to stabilize the patient
- Preeclampsia with HELLP syndrome, do an immediate cesarean section, then start magnesium sulfate post-partum
- Preeclampsia with severe features, start alpha-methyldopa
- Eclampsia, start magnesium sulfate and deliver the baby
- Eclampsia, start magnesium sulfate and labetalol
Which of the following is NOT evidence of HELLP syndrome?
- Elevated creatinine
- Elevated lactate dehydrogenase
- Elevated aspartate transaminase
- Elevated alanine transaminase
- Low platelets
Which of the following features distinguishes eclampsia from preeclampsia?
- Seizures
- Proteinuria
- Renal insufficiency
- Headaches
- Blood pressure greater than 160/100
What is the definitive treatment for preeclampsia?
- Delivery of the baby
- Magnesium sulfate
- Anti-hypertensives
- Expectant management
- Anti-epileptics
Author of lecture Gestational Hypertension (PIH), Preeclampsia (Toxemia) and Eclampsia

Veronica Gillispie, MD, MAS, FACOG
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
