Playlist
Show Playlist
Hide Playlist
Stomach Cancer

-
Slides Stomach and Duodenum.pdf
-
Download Lecture Overview
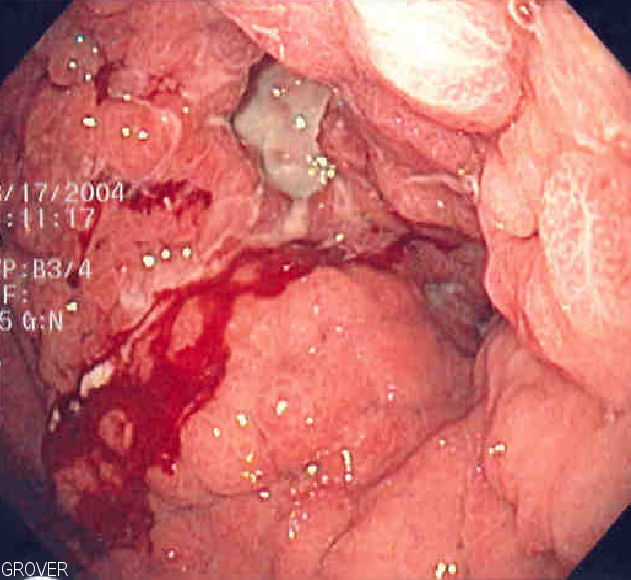
00:01 Gastric Cancer is where we are next. In the United States, there has been a dramatic decrease in adenocarcinoma primarily because, well, we have good proper screening methods in place. 00:14 Our diets, believe it or not, the society is becoming better educated about not consuming nitrates, smoked meats and such. Also, the fact that we have proper regimen for H. pylori eradication. 00:31 Before we move on, there will be two major types of primary gastric cancers or adenocarcinoma and there is one of those lymphomas that we refer to with H. pylori. Highest incidence however definitely Japan. 00:45 And to the point where the government itself is getting involved to properly educate their society so that they are not consuming large amounts of nitrates. Or in other words, to manage and moderate how they prepare their meat. In other words, smoked meat. When you smoke the meat, you are then consuming your nitrates. And the nitrate is extremely carcinogenic. Who is your patient? Male over the age of 50. 01:19 Family history could be associated. And associated with consumption of that smoked meat specifically nitrate. And more likely low socio−economic status as well. Remember, could it also occur in the US? Sure it can. All depends on demographics, population and history, usually the diet comes into play. 01:43 Adenocarcinoma. Here you’ll notice that apart from what may look like a peptic ulcer disease. 01:50 Punched out lesion, but take a look at the margin here. This is inflamed. This is adenocarcinoma. 01:56 You could tell that there is a major abnormal pathologic growth taking place in the stomach and these are rugal folds that you’re seeing more so in the periphery. Adenocarcinoma of the stomach. There are two types. 02:14 The diffuse and the intestinal. H. pylori gives rise to the intestinal and really doesn't metastasize. 02:24 Whereas if it is the diffuse type, it loves to metastasize. You’ve heard of Virchow’s node. 02:30 Painless, left supraclavicular node involvement. You’ve heard of Leser−Trelat sign, which is for example, it literally looks like you’ve taken a piece of chocolate out of your mouth like toffee, placing it on your skin, and that's called Leser−Trelat sign. Seborrheic keratosis. And you’ve heard of Krukenberg tumor of the ovary. 02:50 That is the diffuse type. And molecularly, we had a discussion about E−Cadherin and that would be negative. 02:58 Risk Factors. The H. pylori that might be found with type B chronic atrophic gastritis, you have a phenomenon called Intestinal metaplasia. From henceforth whenever you hear about H. pylori and wherever it loves to live, the type of metaplasia that it’s associated with that you need to know clinically would be intestinal metaplasia. If it’s smoked or salted food, that would be your carcinogen that you’re consuming thus increasing risk of primary gastric adenocarcinoma. Pernicious anemia. 03:37 If you’re thinking about increased pH of your gastric lumen into luminal pH increasing in pernicious anemia, primary atrophic gastric adenocarcinoma may be associated. Post−gastrectomy. Smoking/tobacco use. 04:01 Any time that there is polyps. Now you'll find this to be interesting as well. This is actually a pretty major issue now. Polyps where? These are not polyps in the colon. Is that clear? That is not our topic yet. 04:19 These are the polyps in the stomach. Okay, now that you’ve understood where you are, why am I saying that this is so important in our society now? Tell me about PPIs. Proton pump inhibitors are available over the counter. Prevacid, Prilosec, so on and so forth.You take PPIs and patients do this quite a bit. 04:43 And the patient, if they are not able to properly monitor how much PPI that they are taking because their friends told them, "Oh, I’m having heartburn, take PPI, take PPI, take PPI". 04:52 So we have now patients, many more of them, that are taking PPIs. Okay, great. No, not really. 05:01 Because if acid is being diminished so very much in these patients taking PPI, what’s the feedback for acid? Gastrin. If the gastrin levels are low, excuse me, acid levels are low, what’s my gastrin level? High. Tell me about the physiology of gastrin. Sure, it works on parietal cell. Sure, it is one of the most important stimulators of acid secretion. In addition, isn’t gastrin responsible for proper development of the mucosa? And in fact if you have too much gastrin, couldn't you result in hypertrophy? And perhaps increased growth of your gastric tissue? There you go. Therefore with PPIs, with the increased growth that might be taking place due to gastrin, you are developing or the patient is developing polyps within the stomach. Any time that you have such abnormal proliferation of cells and such, you’re always increasing the risk of dysplasia. And with that dysplasia, you’re worried about perhaps going on to adenocarcinoma. 06:21 That’s your full story for that second bullet point which you should fully understand. It’s pharm, physio, and here, the pathology. Familial polyposis. Familial polyposis, we had that discussion in neoplasia with Familial adenomatous polyposis. And with familial adenomatous polyposis, we've talked about APC gene mutation, beta catenin, Wnt. And you could have polyposis up and down the alimentary canal. 06:53 Low consumption of fruit and vegetable. So we have a high fat, low vegetable, low fiber diet. 07:01 All contributing to cancer in general, in the GI tract. Not only colorectal cancer. Seing my risk factor there. 07:10 High fat, low fiber but then also gastric adenocarcinoma. Let’s talk about your clinical presentation of Gastric Cancer. Abdominal pain, weight loss, bleeding. You’re causing damage. I showed you a picture on gross examination of the wall of the stomach that has now been compromised. Erosion, loss of blood, iron deficiency anemia. Epigastric mass. The patient will tell you, "Doc, I’m not hungry" or "I eat food and I get satiated very quickly". And weight loss and older patient and history of maybe pernicious anemia, maybe smoked meats or H. pylori, concerning. 07:58 If it is the gastric cancer that likes to spread. Where does it like to spread? It loves to maybe perhaps spread to the left supraclavicular lymph node. Left. This is called your Virchow’s node. 08:13 Maybe hematogenously. Hematogenenously, not seeding. From your stomach and you then spread to the ovary. 08:23 These are called Krukenberg tumor and you would then expect to find signet ring cells. This is all part of your diffuse type of primary gastric adenocarcinoma. 08:35 A Krukenberg tumor in a 34-year-old woman in stomach cancer you’ll notice that in the ovary you find number of tumors and nodules representing metastasis hematogenously from the stomach down into the ovaries. 08:54 And upon histologic examination, you would expect to see a signet ring cell. 09:04 Management. What do you want to do? Endoscopy. Remember, endoscopy not only do you check out the esophagus, you do esophagogastroduodenoscopy. The whole bit, upper. Endoscopy will show gastric mass or an ulcer with heaped-up margin. Not punched-out lesion. A clean punched-out lesion to you upon description is peptic ulcer disease. The heaped-up and I showed you a picture of exactly what I said, around it there is increased proliferation. Total gastrectomy to localized disease. Chemotherapy and radiation, may be used for palliation. Responses not good though. That's not good. The 5−year survival rate drops from 90% for early gastric cancer to 10% for lymph node involvement. So what the heck does that mean to you? You want to make sure that you’re extremely vigilant about who your patient is. 10:08 Surveillance programs in China and Japan for the exact reason. Because if you catch your patient and then the patient says, “Doc, I have a lump on my neck." "Does it hurt?" "No." "Oh my goodness". 10:21 You see what I’m saying. You just drop from 90% of survival 5-year, dropped to 10% because now if there is lymph node involvement, that means metastasis has now begun. Your patient, high, high risk for mortality.
About the Lecture
The lecture Stomach Cancer by Carlo Raj, MD is from the course Stomach and Duodenum Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following organisms is associated with adenocarcinoma of the stomach?
- H. pylori
- HIV
- HPV
- Shigella
- Salmonella
Which of the following is a predisposing dietary factor for adenocarcinoma?
- Salt-preserved food
- Sweet food
- Bitter food
- Sour food
- Acidic food
Which of the following anemias is a predisposing factor for adenocarcinoma?
- Pernicious anemia
- Hypochromic anemia
- Myeloid anemia
- Sickle cell anemia
- Iron-deficiency anemia
Which of the following is a possible symptom of gastric cancer?
- Reduced hunger
- Increased hunger
- Increased salivation
- Faster gastric emptying
- Slower gastric emptying
Author of lecture Stomach Cancer

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
very well explained. I would recommend this lecture to any medical student. I enjoyed every bit of it.
