Playlist
Show Playlist
Hide Playlist
Fetal Alcohol Syndrome (FAS)

-
Slides FetalAlcoholSyndrome Pediatrics.pdf
-
Download Lecture Overview
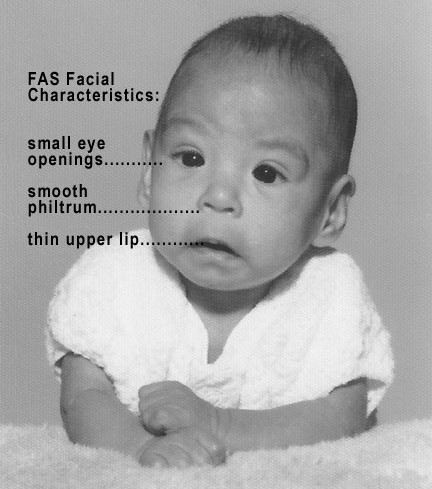
00:01 In this lecture, I'm going to review fetal alcohol syndrome. 00:04 It's not a genetic syndrome. 00:07 Well, maybe it is a little bit in that alcoholism is a little bit genetically inherited but it's not a genetic syndrome because these patients acquire this disease as a result of exposure in utero to alcohol that the mother drinks. 00:21 The reason I'm bringing it up in the genetics course is because it presents with such syndromic features that it's often mistaken as a genetic syndrome and people call geneticists to make this diagnosis. 00:35 So, let's go through it. 00:38 Fetal alcohol syndrome occurs in roughly 1% of all live births in the United States. 00:44 You think that's a lot. It is a lot. It's way too many. 00:48 But the disease does have variable penetrants depending on the degree of exposure and also the underlying genetics of the child, so it's somewhat hard to really know for sure what this rate is. 01:00 This is the most common cause of teratogenic intellectual disability in the United States. 01:06 The risk increases in certain circumstances. 01:11 Patients are more likely to have infants who are born with fetal alcohol syndrome if these women have a high-dose exposure in utero. 01:22 So, with a blood alcohol level of more than 150mg/dl, that infant is at increased risk for exposure. 01:30 It's hard to really correlate that with how many drinks but if a patient is drinking more than 2g/kg/day of alcohol, that's gonna be a problem. 01:40 It's also associated with binge drinking. 01:43 In patients who don't drink much on the weekdays but then get a little bit drunk on the weekends, there's a concern. 01:50 People with alcohol use disorder have a 30 to 50% chance of having a child born with multiple problems with fetal alcohol syndrome. 01:58 Alcoholism is a bad disease and when they get pregnant, their children are at substantial risk. 02:04 So, how does it happen? Alcohol crosses the placenta and reaches the fetus. 02:11 The fetus needs the mother's hepatic detoxification. 02:15 Infants don't have alcohol dehydrogenase activity in their fetal liver. 02:21 So, it's really the mother's clearance of the drug that the fetus is requiring. 02:25 The amniotic fluid though, acts as a reservoir for alcohol. 02:31 So, while the mother may clear it from her system, it's going to persist in the amniotic fluid and these infants get prolonged fetal exposure of alcohol. 02:42 And remember ethanol and its metabolite acetaldehyde will alter fetal development. 02:49 So, it's not just ethanol, it's also its next metabolite, acetaldehyde. 02:54 So how do these children present? Well, they may have shortened palpebral fissures. 03:00 The palpebral fissure remember is just the opening of the eye and it can be a bit shorter. They may have a flattened mid face. 03:07 They may have a long and flat philtrum. 03:10 The philtrum remember is those 2 little lines under the nose. 03:13 It will be a little flattened so you almost can't see them and a little bit longer. 03:17 And they may have a thin upper lip or a thin vermilion border on the upper lip. 03:22 So, a long flat philtrum and a thin upper lip, and then the flattened mid face and the shortened palpebral fissures. 03:30 The nose may also angle a little bit up. 03:32 So here's some examples of patients with fetal alcohol syndrome. 03:37 You can see these patterns on all these children. 03:41 So, what else can go wrong? If it's just a problem with the face, why are we so worried? Well, these children will typically have growth retardation. 03:51 Their birth weight will be low and they will have a decelerating weight gain and they will have a thin body habitus. 03:58 They can have brain abnormalities, structural brain abnormalities such as microcephaly or even an absent corpus callosum or a reduced generation of a cerebellum. 04:12 They can have structural problems that can cause significant neurologic disease. 04:17 They may have cognitive abnormalities as well with poor impulse control, attention deficit or attention deficit hyperactivity disorder, they may have language deficits, and they may be less capable of doing math. 04:31 And, these patients may have birth defects such as congenital heart disease or urinary tract abnormalities. 04:38 And lastly, they may have extremity defects. 04:41 You may see the hockey-stick crease which is an angular crease in the shape of a hockey stick on the palm, and they may have small distal phalanges. 04:51 So how do we treat these patients? Well, we have to fix any congenital heart disease or anything else that's going on, but the mainstay of therapy is intervention in terms of behavior and intellectual development. 05:05 We need to get these kids plugged in to early intervention so they can maximize their young childhood intellectual development. 05:13 We need to put them in programs like Head Start and get them into good schools with good programs and to find them individual learning plans that work for the family. 05:21 Also, it's critical to counsel families about prevention. 05:26 We need to talk to parents about how they can prevent future pregnancies from also having fetal alcohol syndrome. 05:34 We need to counsel women to avoid drinking while pregnant. 05:37 So that's my review of fetal alcohol syndrome. 05:41 Thanks for your time.
About the Lecture
The lecture Fetal Alcohol Syndrome (FAS) by Brian Alverson, MD is from the course Pediatric Genetics.
Included Quiz Questions
Which of the following is NOT a finding in fetal alcohol syndrome?
- Macrocephaly
- Growth retardation
- Cognitive abnormalities
- Congenital heart disease
- Urinary tract anomalies
Which of the following is NOT a characteristic facial feature of fetal alcohol syndrome?
- Long nose
- Thin upper lip
- Flat midface
- Short palpebral fissures
- Indistinct philtrum
Which of the following is true regarding fetal alcohol syndrome?
- It can develop with binge drinking.
- It only results from chronic long-term maternal exposure to alcohol.
- Alcohol does not cross a healthy placenta.
- Amniotic fluid detoxifies alcohol.
- Alcohol dehydrogenase activity is maximum in the fetal liver.
A pregnant woman occasionally consumes moderate amounts of alcohol. Which of the following contributes to sustaining a toxic environment for the fetus in this patient?
- Amniotic fluid
- Maternal alcohol dehydrogenase
- Maternal kidneys
- Maternal liver
- Fetal alcohol dehydrogenase
Which of the following is not a feature of fetal alcohol syndrome?
- Macrosomia
- Attention deficit hyperactivity disorder
- Congenital heart disease
- Hockey stick palmar crease
- Microcephaly
Author of lecture Fetal Alcohol Syndrome (FAS)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
