Playlist
Show Playlist
Hide Playlist
Familial Adenomatous Polyposis, Gardner's Syndrome and Turcot Syndrome


-
Slides Small and large bowel.pdf
-
Download Lecture Overview
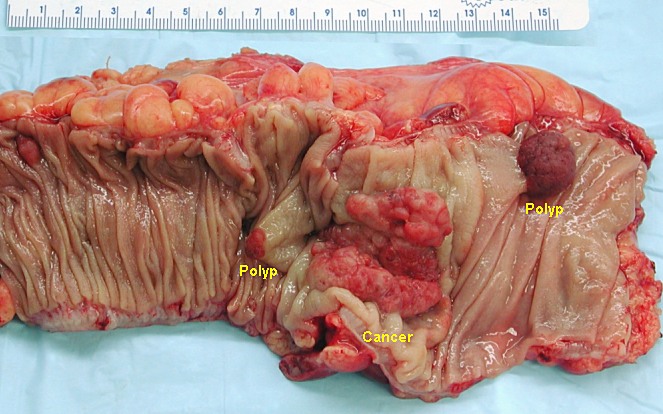
00:00 HMPCC associated with hereditary nonpolyposis syndrome. 00:06 That is the one which where we talked about when you have right colorectal cancer. 00:10 Meaning of FAP, familial adenomatous polyposis. Autosomal dominant. 00:16 It is a carpet of polyps. This is a young patient and there is going to be 100% chance of going on to colorectal cancer. 00:25 Screening for all members and you do prophylactic colectomy because you know your patient is going on to colorectal cancer. What kind? Left sided. Memorize that, if you haven`t all ready. 00:37 The full molecular talk about a neoplasia. 00:41 Once again, familial adenomatous polyposis. 00:44 You must know about APC, adenomatous polyposis coli, which then controls your beta-catenin. And if your APC has been lost, your beta-catenin is an opposed and brings about excessive transcription. 01:00 With all that transcriptions taking place within your intestinal epithelial cell, you can only imagine that you are going to form carpets of polyps. 01:09 APC, beta-catenin and WMT, all properly regulate your growth and proliferation of your epithelial cell. 01:20 If it is FAP and you have other associations for example, if it is going to be extra intestinal referring to your: S, sebaceous on your skin, O, osteoma a benign bone tumor; D, desmoid and that would be a fibroma and now you called this Gardner´s syndrome. 01:45 Gardner´s syndrome. If you have FAP associated with Turcot, C as in Turcot, you may use this with CCNS, a glioma. 01:58 So you have FAP plus a glioma, you call this Turcot, if you have FAP with your sebaceous osteoma and desmoid, this is then known as your Gardner. 02:10 If you forgotten any component that I have just mention here, for either of the two, please repeat what I just said and make sure that you have firmly implanted those facts into your head. 02:21 So that you know the variants of your familial adenomatous polyposis. 02:24 All of these would be hereditary polyposis syndrome. 02:28 Hereby if you're nonpolyposis also also called Lynch and with HNPCC, this will be on the right side and you have ovarian issues as well. 02:38 Take a look at this. We have a carpet of polyps, either with a colonoscopy, where you find so many polyps and then you open up the colon and when you do so, you find a carpet of polyps on your right. 02:56 Hence, 100% risks of going all to colorectal cancer. 03:01 This has nothing to do, in by that I mean the following. 03:05 You are not going to waste your time trying to figure out what kind of polyp, when he haves so many different polyps, a hundreds and thousands of them. 03:12 You're going on to colorectal cancer. So take it out. Don´t waste time. 03:16 Whereas if you have individual polyps, that's when you start paying attention to, is this villous or tubular. 03:23 Villous or tubular? If it's tubular, it still will be taken out. 03:27 You clip it, but the risk of going on to colorectal cancer technically is decreased. 03:32 Whereas if it's villous, it's the villain, at flat, but it does not being shown here. 03:38 But that has an increase risk of colorectal cancer.
About the Lecture
The lecture Familial Adenomatous Polyposis, Gardner's Syndrome and Turcot Syndrome by Carlo Raj, MD is from the course Small and Large Intestine Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
What percentage of patients presenting with FAP subsequently develop colon cancer?
- Almost 100%
- Almost 60%
- Almost 50%
- Almost 40%
- Only 10%
Which of the following proteins is involved in the pathogenesis of familial adenomatous polyposis?
- Beta-catenin
- ICAM
- E-cadherin
- LFA-3
- PECAM
Which signal transduction pathway is involved in FAP syndrome?
- Wnt pathway
- Tyrosine kinase pathway
- K-Ras signaling pathway
- Cyclic AMP pathway
- MAPK signaling pathway
A patient presents with a history of being diagnosed with a desmoid tumor. The doctor says the X-ray of his knee shows an expansile bone tumor. The doctor also notices multiple sebaceous cysts. Which of the following is this presentation associated with?
- Hereditary polyposis
- Hereditary colon cancer
- Hereditary endometrial cancer
- Hereditary gastrointestinal stromal tumors
- Hereditary gastric adenocarcinoma
Which of the following is NOT seen in Gardner syndrome?
- Non-melanoma skin cancer
- Multiple polyps
- Multiple sebaceous cysts
- Osteoid osteomas
- Desmoid fibromatosis
Which of the following regions is NOT prone to the development of colon cancer in a patient with FAP?
- Ileocecal junction
- Sigmoid colon
- Rectum
- Splenic flexure
- Rectosigmoid junction
Which brain tumor is associated with Turcot syndrome?
- Glioma
- Astrocytoma
- Pinealoma
- Meningioma
- Acoustic neuroma
Author of lecture Familial Adenomatous Polyposis, Gardner's Syndrome and Turcot Syndrome

Carlo Raj, MD
Customer reviews
2,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
not sure how to connect some things or how they link up. just difficult to follow and conceptualise
