Playlist
Show Playlist
Hide Playlist
Hypertrophic Cardiomyopathy: Etiology and Variants

-
Slides Cardiomyopathy.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
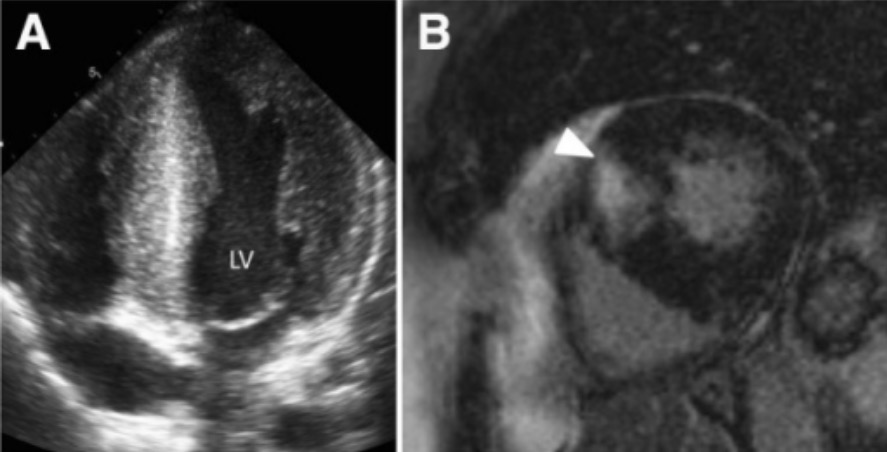
00:01 Let's go to the next one. 00:02 Less common, still an important cause, genetic cause of cardiomyopathy. 00:08 And it's the flip side of the coin. 00:09 Remember dilated cardiomyopathy - floppy heart, poor systolic function. 00:14 Hypertrophic cardiomyopathy - really thick muscle, you know, well, muscled heart doesn't relax. 00:22 Okay? So it's a diastolic dysfunction, there's impaired left ventricular relaxation and filling, and that can be as bad as poor left ventricular ejection fraction. 00:34 What we see grossly is that there's a thick walled heavy and hypercontractile heart. 00:41 The mutations that cause this tend to make the sarcomere squeeze more efficiently, but relax more poorly. 00:50 The systolic function is usually preserved. 00:52 If anything, it may be increased. 00:54 So in dilated cardiomyopathy, we're talking about ejection fractions of 20 to 30%. 00:59 The systolic function in a hypertrophic cardiomyopathy can be 60, 70, sometimes even 80%. 01:04 So we're squeezing very aggressively. 01:08 The mutations for the most part, the vast majority, and this is what will be on the boards, you don't have to remember a lot of the exceptions. 01:15 Most mutations will involve the myosin heavy chain. 01:19 So it's indicated here as an X, we actually don't delete it. 01:23 We have mutations in it so that the heads of the myosin heavy chain bind with greater affinity to the actin light chain, and we get hypercontractile forces generated. 01:37 So that's the majority of them. 01:38 There are other mutations, as we'll briefly mention later on. 01:42 The hypertrophy is most apparent within the left ventricle. 01:49 It is also happening within the right ventricle. 01:51 But it's the left ventricle that squeezes most vigorously in the first place, and so it's going to be the one that we're going to see most of the effects. 01:59 So there's something called asymmetric septal hypertrophy, where there is a more prominent septal hypertrophy compared to the left ventricular free wall. 02:08 And you see there, the septum is markedly thickened, that gives the ventricular cavity a banana-like configuration. 02:16 This septal hypertrophy impinges on the left ventricular outflow and the aortic valve there is actually can be somewhat compromised as we'll show in a subsequent set of slides. 02:27 So it can be an obstructive cardiomyopathy, typically with asymmetric septal hypertrophy. 02:33 You can also have concentric hypertrophy, which is the less common kind of variant, where the entire wall is relatively thickened. 02:42 The ventricular chamber is smaller because the wall has gotten much thicker. 02:47 It also doesn't relax at all well, so that chamber remains reasonably small. 02:52 This concentric hypertrophy is less likely to have left ventricular outflow tract obstruction, and it doesn't really have that same banana-like configuration, but it's a non classic variant of hypertrophic cardiomyopathy. 03:07 So the non-obstructive hypertrophic cardiomyopathy occurs in about 65 to 75%. 03:15 It's shown here, as that septal hypertrophy. 03:19 You can still have septal hypertrophy without actually formally having outflow tract obstruction. 03:25 But if we're going to get outflow tract obstruction, it's going to be with this asymmetric hypertrophy of the left ventricle. 03:33 With the obstructive form, which is roughly a third of these asymmetric septal hypertrophy, the involvement of the interventricular septum increases more and more and more, and now we are compromising the outflow through the aortic valve. 03:48 So this is going to be obstructive hypertrophic cardiomyopathy or hypertrophic obstructive cardiomyopathy called HOCM Alright, and that is a very dynamic left ventricular outflow tract with an obstruction. 04:02 So let's look at a little bit more detail when we talk about obstructive cardiomyopathy or hypertrophic obstructive cardiomyopathy or HOCM. 04:10 You can see that as the septum gets thicker and thicker and thicker in the asymmetric septal hypertrophy setting, we will now impinge on the outflow tract because the anterior mitral leaflet, gets pulled by turbulence by a hyperdynamic flow going out the left ventricular outflow tract and will get pulled towards the septum. 04:35 This gives us what is called systolic anterior motion of the mitral leaflet that is seen on echocardiogram, and that gives us this premature closure of the left ventricular outflow tract is that anterior leaflet as pulled up against the septum. 04:52 We can see that grossly when we're holding the heart in our hands as a plaque of fibrous connective tissue, intimal hyperplasia where the anterior leaflet has slapped up against the interventricular septum over and over and over again. 05:07 And this is where we get that obstructive cardiomyopathy result. 05:12 So it causes left ventricular outflow tract obstruction with premature closure of the left ventricular outflow tract. 05:17 And we will get because of that slapping motion and the trauma associated with that, we will get overall thickening of the mitral leaflet. 05:25 Because the mitral valve is now being pulled towards the septum during systole, that means, as the heart squeezes very hyperdynamically, we're going to have retrograde regurgitant flow back out through the mitral valve apparatus. 05:45 So hypertrophic obstructive cardiomyopathy has diminished left ventricular outflow, premature closure, damage to the mitral valve, anterior leaflet and regurgitant flow so you can have significant heart failure in that setting.
About the Lecture
The lecture Hypertrophic Cardiomyopathy: Etiology and Variants by Richard Mitchell, MD, PhD is from the course Cardiomyopathy.
Included Quiz Questions
What is the most common etiology of hypertrophic cardiomyopathy?
- A mutation affecting the thick myofilament proteins
- A mutation affecting the thin myofilament proteins
- A mutation affecting the DNA single-strand break repair pathway
- A mutation affecting the DNA double-strand break repair pathway
- A mutation affecting the calcium channels
What is hypertrophic cardiomyopathy?
- Thickening of the heart muscle leading to diastolic dysfunction with impaired ventricular relaxation and filling
- Thickening of the heart muscle leading to systolic dysfunction
- Thickening of the heart muscle leading to electrical dysfunction and delayed closure of the left ventricular outflow tract
- Thickening of the heart muscle leading to impaired atrial filling
- Thickening of the pericardium that leads to diastolic dysfunction with impaired ventricular relaxation and filling
What causes ventricular outflow tract obstruction in patients with hypertrophic cardiomyopathy?
- A thick anterior mitral leaflet contacts the septum during systole to prevent blood outflow.
- A thick posterior mitral leaflet contacts the septum during systole to prevent blood outflow.
- A thick anterior mitral leaflet contacts the septum during diastole to prevent blood outflow.
- A thick posterior mitral leaflet contacts the septum during diastole to prevent blood outflow.
- A thick anterior pulmonary leaflet contacts the septum during systole to prevent blood outflow.
Author of lecture Hypertrophic Cardiomyopathy: Etiology and Variants

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
