Playlist
Show Playlist
Hide Playlist
Esophagitis

-
Slides GIP Esophagitis.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
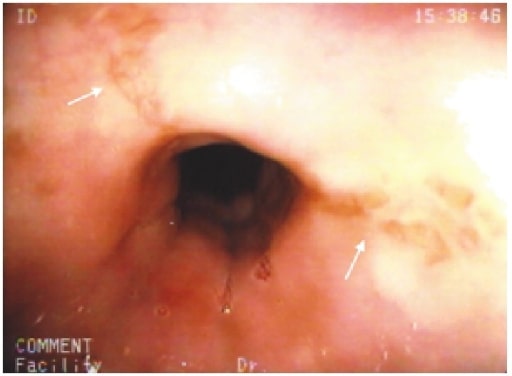
00:01 All right. So let's for this talk, talk about esophagitis. 00:06 Literally, it's inflammation of the esophageal mucosa, so itis of the esophagus. 00:11 So causes or etiology for esophagitis. There are four basic categories that we can think about. 00:19 One is gastroesophageal reflux disease or GERD and that's where we bathe the lower portion of the esophagus in gastric acidity, hydrochloric acid in the pH of two. 00:32 We've covered that in excruciating detail in another talk. 00:37 So I'll refer you back to the GERD talk if you wanna learn more about that. 00:41 We're gonna focus on the next three as causes of esophagitis. 00:44 So medication-associated esophagitis, infectious associated esophagitis, mostly viruses, but occasionally, fungus, and the eosinophilic esophagitis which is its own distinct entity. 00:57 Of the medication-related esophagitis, antibiotics and anti-inflammatory are probably the major bad actors. 01:06 So certain antibiotics, tetracyclines and clindamycin can cause, idiosyncratically in some people, esophagitis. 01:13 Also, if you do not take these oral antibiotics with sufficient fluid, their mechanical kind of stickiness can make them stick within the lower esophageal segment and you can get a direct inflammation associated with them. 01:28 The anti-inflammatories, the non-steroidal anti-inflammatory drugs or NSAID's you would think would be, "Gee, anti-inflammatory." But in fact, they also regulate the microvascular flow within the esophagus in the stomach and if you take too many, it can actually lead to ischemic esophagitis. 01:49 Bisphosphonates such as alendronate which is used in the treatment of osteoporosis can also in some patients, in many patients actually, cause irritation of the lower esophageal segment. 02:02 And then potassium chloride, quinidine, iron supplements, there are many that can potentially be irritating or cause inflammation of the esophagus. 02:10 With regard to infectious causes, cytomegalovirus and herpes simplex virus are probably the most common but candidiasis, particularly, in the immunocompromised host is also a major cause of esophagitis. 02:23 And then, a special entity of eosinophilic esophagitis. 02:27 In some patients, relatively infrequently, but there can be an antigen sensitization through foods or aeroallergens that are inhaled down the esophagus. 02:38 And an induction of a hyper-sensitivity response with eosinophilia and associated inflammation leading to esophageal dysfunction. 02:48 This entity, while fairly rare, does happen and if we're looking for a particular population, it's typically young, Caucasian men in their 20's. 02:59 Just to give you a sense of what this looks like and then, we won't talk anymore about it, this is eosinophilic esophagitis. 03:04 This is a biopsy with a transmural piece of the epithelium showing a stratified squamous, non- keratinizing epithelium with scattered eosinophils throughout and that's how we would make the diagnosis. The pathophysiology. 03:19 Basically, we have all the various causes. We have medication, we have infections, we have reflux, we have eosinophils causing the release of cytokines and other inflammatory mediators in the epithelium and in the sub epithelial connective tissues in the esophagus. 03:40 That inflammation will lead to edema which in many ways, can compromise the vascular flow, so we can even have erosions. 03:51 The inflammatory mediators can cause loss of epithelium, so we can get sloughing. 03:55 The edema will cause luminal narrowing. 03:58 So the clinical presentation for esophagitis can be painful swallowing, odynophagia or just difficulty swelling, dysphagia. 04:09 There could be a sense of heartburn. Where we have irritation of the lining, on the esophagus and causing them the nerves in that area to register as irritation. 04:23 And then, retrosternal pain. So it can be more than just a burn, it can be pain. 04:28 The diagnosis is largely clinical but to nail the diagnosis, we need to do endoscopy. 04:34 This is just giving you a sense of some of the views that the gastrointestinal endoscope can see when we are in the setting of esophagitis. 04:44 On the left-hand side is a medication that induces esophagitis, somewhat non-specifically, there can be some erythema, some redness, at the lower esophageal sphincter. 04:53 But the rest of the mucosa looks largely intact may have focal erosions as you see at the bottom of the picture. 05:00 At the right-hand side is a good example of candida esophagitis in an immune compromised host and we have this fluffy, white layering of the candida of hyphae all over the surface of the esophagus. 05:14 Cytomegalovirus, relatively non-descript as you see there on the left, but there is definitely erythema and there is definitely edema. 05:22 And on the right, a very characteristic look of eosinophilic esophagitis with kind of that layering that you see there and that's quite typical of that entity. 05:32 How do we manage it? So for reflux disease, we're gonna treat it as we would for gastroesophageal reflux disease. 05:38 And we will do simple things like sitting up, not eating before bedtime, and medications that will reduce the gastric acidity. 05:49 For medication related, gee, let's stop the medication and it may take a little bit of trial and error before we find the right one on patients who are on multiple drugs but that will definitely help. 06:01 For infectious causes of esophagitis, let's treat it or if it's an immunocompromised state, we need to get them out of that state. 06:10 So if they're getting chemotherapy, if they have HIV/AIDS, we know what we need to do. 06:15 And for eosinophilic esophagitis, you can give topical or systemic steroids that will reduce the inflammation. 06:21 And for almost all of these, you would want to give a proton pump inhibitor to reduce the gastric acidity. 06:28 Major complication of this is that with recurrent injury and recurrent inflammation, we will get recurrent scarring of the esophagus which will lead to structuring which will lead to dysphagia over the long-term. 06:44 We'd like to try to avoid that if we can. And with that, esophagitis.
About the Lecture
The lecture Esophagitis by Richard Mitchell, MD, PhD is from the course Disorders of the Esophagus.
Included Quiz Questions
What is one of the most common causes of medication-induced esophagitis?
- NSAIDs
- Antivirals
- PPIs
- Beta-blockers
- Alpha agonists
What is one of the most common causes of infectious esophagitis?
- Cytomegalovirus
- Human papillomavirus
- Varicella zoster virus
- Staphylococcus aureus
- Respiratory syncytial virus
What is an important component in the management of eosinophilic esophagitis?
- Steroids
- Antimicrobials
- Medication discontinuation
- Antifungals
- Silver sulfadiazine
Author of lecture Esophagitis

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
4 customer reviews without text
4 user review without text
