Playlist
Show Playlist
Hide Playlist
Esophageal Diverticula

-
Slides GIP Esophageal Diverticula.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
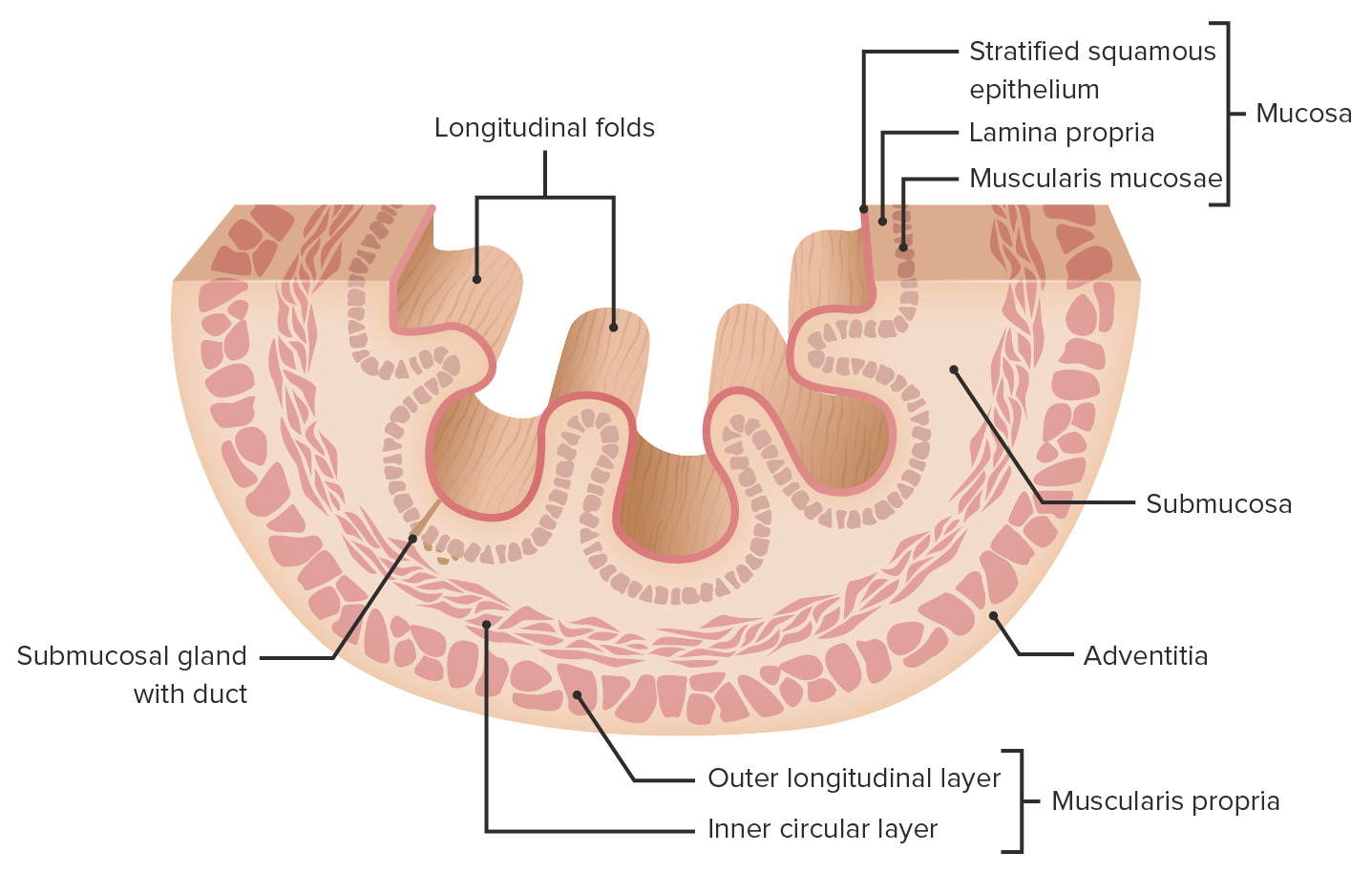
00:01 Welcome. In this talk, we're gonna cover esophageal diverticula or outpouchings of the esophagus. 00:08 An esophageal diverticulum, singular, or diverticula, plural, are sac-like protrusions of the bowel wall. 00:16 The epidemiology is reasonably straightforward but you need to understand that there are three different locations where esophageal diverticula typically occur. 00:27 All of them are more common in older individuals such as myself. 00:31 The most common overall is the Zenker diverticulum which is going to be very proximal. 00:38 It's going to be a retroesophageal outpouching. 00:42 So it goes backwards from the esophagus. 00:46 We'll come back to why it occurs at this location in the nature of how it's composed. 00:52 The second most common form is at kind of where the trachea bifurcates into the bronchi and at that location, there are a number of fibrous connective tissue ligaments and other elements that can pull traction and ultimately, lead to the formation of a diverticulum at that rough location. 01:13 Or at the point where the esophagus crosses the diaphragm and enters into the stomach just above the diaphragm, you can also have protrusions of the esophagus at that location. 01:27 The Zenker diverticulum, the most common form, happens at that particular location there in the Killian's triangle. 01:35 Superior to that is the thyropharyngeal part. That's the thyropharyngeus muscle. 01:40 Distal to that is the cricopharyngeus muscle and there's a gap between those two muscle bundles. 01:46 If the cricopharyngeus muscle spasms too much, then you cause increased pressure within the lumen of the esophagus and you can get an outpouching. 01:59 Similarly, when we look more distally for example, at the diverticulum that can occur just above the diaphragm, that can be because the lower esophageal sphincter causes too much intraluminal pressure with an outpouching on that location. 02:14 So the pathophysiology of esophageal diverticulum is reasonably straightforward but we need to have one point of nomenclature very clear. 02:23 So throughout the GI tract, there are three basic layers. 02:27 There's the mucosa lined by epithelium that surrounds the lumen. 02:31 Deep to that is the submucosa, and then, we're into the muscularis propria or the muscle proper lined on the outside by the serosa which forms part of the adventitia. 02:42 In a true diverticulum, all three layers of the wall pouch out. 02:48 So we have a protrusion of all three layers. 02:51 The mucosa, the submucosa and muscularis propria. 02:57 With a false diverticula, we have not a complete lining of the smooth muscle of the muscularis propria. 03:05 So it is not a complete or true diverticulum. 03:10 So of the three kinds of diverticulum in the different locations, more proximal, more midline, and more distal, the Zenker's diverticulum is a false diverticulum. 03:20 Again, that's the cricopharyngeus muscle squeezing and there is an outpouching but it's not completely lined by the muscularis propria. 03:27 In the lower esophageal or mid kind of mid-zone diverticulum, it's a true diverticulum. 03:33 All three layers are pulled out and again, this is due to traction from associated connective tissue. 03:39 And the lower esophageal diverticulum tends to be a weakness, a focal weakness of the wall and again, a false diverticulum. 03:46 The clinical presentation is actually kind of interesting. 03:48 So there may obviously be difficulty swallowing. 03:51 You can have these pouches and they may interrupt the normal flow in the swallowing mechanism. 03:58 There may be halitosis, meaning, bad breath. 04:01 And that's because food and bacteria get caught in these pouches and they - there's fermentation that's going on that then gets exhaled back out and foul - it smells like foul breath. 04:13 Regurgitation, clearly, all that food is in there and it doesn't always have to go down. 04:18 So if the pouch dumps its content back - contents back into the esophagus, it can come up and you can have regurgitation. 04:27 Clearly, the contents may inappropriately go down the wrong way and into the trachea so that you get aspiration. 04:35 And while eating, again, you may have regurgitation so that there is a couching sensation with food coming in the reverse direction. 04:43 Because of the size with very large diverticula, you can have actually compression of nerves and other structures. 04:52 So you can get retrosternal pain and pressure. 04:55 And you may actually feel or have a palpable neck mass because these can eventually lead to severe dysphagia. 05:03 Patients who have very severe diverticula can ultimately experience weight loss. 05:10 So that's your clinical presentation. 05:12 Making the diagnosis formally is reasonably straightforward. 05:15 So if you put down a fiber optic endoscope, you can see the outpouching in one of those three general locations. 05:22 You can also do a barium swallow. 05:24 And so what's being demonstrated here is a rather large diverticulum, more proximal associated with the Killian's triangle and you're seeing it filled up with barium, so this would be a rather large diverticulum that would be palpable probably even as a neck mass. 05:42 So how do we manage these? There could be medical treatment. 05:46 Mostly, these are to limit the extent of reflux or damage associated with reflux and particularly, for the diverticula that occurs near the diaphragm. 05:59 We would give proton pump inhibitors to minimize gastric acidity reflux. 06:04 You can also inject botulinum toxin, either more proximal, midline, or distal to limit the abnormal squeezing of the smooth muscle that may exacerbate the formation or the expansion of the diverticula. 06:18 And finally, if these are not sufficient or if they're rather large diverticulum requires surgery where we literally excise the outpouching and then sew it back up. With that, we've covered diverticula within the esophagus.
About the Lecture
The lecture Esophageal Diverticula by Richard Mitchell, MD, PhD is from the course Disorders of the Esophagus.
Included Quiz Questions
What is the location of Zenker diverticulum?
- Killian triangle
- Cricopharyngeus muscle
- Cricoid cartilage
- Arytenoid cartilage
- Posterior pharyngeal wall
What is NOT a typical symptom of esophageal diverticula?
- Abdominal distension
- Dysphagia
- Halitosis
- Regurgitation
- Aspiration
What is a medication used to manage esophageal diverticula?
- Botulinum toxin
- NSAIDs
- Warfarin
- Steroids
- Carafate
Author of lecture Esophageal Diverticula

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
