Playlist
Show Playlist
Hide Playlist
Erythema Multiforme

-
Slides Dermatology Inflammatory Skin Diseases.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
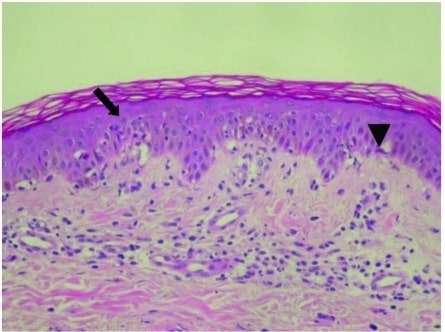
00:02 Here, we’ll take a look at erythema multiforme. 00:06 As we walk through this, you’ve heard of the term erythema quite a bit, and it would be in your best interest to, every once in a while, just come back and make sure that you’re extremely aware of some of the important erythemas that you must know for your boards and wards. 00:24 Erythema nodosum, erythema multiforme, which is our topic here, erythema migrans or erythema migran chronicum, your target lesion. 00:35 And then you have your erythema marginatum. 00:38 That might be part of your Jones criteria for? Good, rheumatic fever. 00:44 Repeat what I just said. 00:46 Make sure you know those four in and out. 00:49 Our topic here, erythema multiforme. 00:53 Where are you going to find these lesions and what are they? Allow the name to speak to you. 00:59 You’re going to find multiple concentric erythematous rings. 01:04 Where and how and why? Let’s take a look. 01:08 It can be a reaction to infection or medication. 01:11 Infection, let me give you one. 01:13 Multiforme, M, multiforme, M, what’s the most common cause of atypical pneumonia? Mycoplasma pneumonia, as an example of an infection, then resulting in a trigger or being a trigger for erythema multiforme, or usual suspect for medications include antibiotics such as sulfonamides. 01:41 Let’s continue. 01:43 Is this going to kill you? Thank goodness no. 01:47 Erythema multiforme minor is highly associated with HSV infection, herpes simplex virus. 01:53 It usually involves the hands and the feet, dusky plaques. 01:59 Now, you get into more serious condition. 02:02 Minor is not going to kill you, luckily. 02:05 However, you'll notice this and you’re definitely worried about, maybe perhaps, major. 02:11 Another name for erythema multiforme, EM major, is Stevens-Johnson syndrome. 02:18 Oh, boy. 02:20 So, this is the story that you want to take with you, or the spectrum on this slide is what? You’re going from minor to major, and as you become more and more severe, increased risk for mortality. 02:34 I’m being very dramatic here because I need you to understand the theme of this page. 02:40 Erythema major, Stevens-Johnson syndrome, more severe. 02:43 It involves at least two mucosal surfaces. 02:47 Then we have extremely dangerous to the point where your patient -- It just looks like death, let me tell you. 02:56 Toxic epidermal necrolysis. 02:59 You have, what happens for the most part, greater than 30% of your body is undergoing necrotic changes of the skin. 03:08 Thirty percent, it’s almost like having a third-degree burn. 03:12 Is this clear? So, we have a spectrum. 03:17 Erythema multiforme minor, think of infections such as HSV, mycoplasma pneumonia, antibiotics such as sulfonamides. 03:23 Major, Stevens-Johnson syndrome, and that in which you have greater than 30% of your body that’s involved. 03:31 It will be toxic epidermal necrolysis. 03:35 And here are divisions that you very much want to keep in mind between Stevens-Johnson and TEN, toxic epidermal necrolysis. 03:44 Let’s take a look at the morphology of erythema multiforme. 03:48 We have a picture in which I’m showing you in the mucosal region and on the hard palate on top, we have erythematous multiforme. 03:57 And then we have a second picture in which we see a concentric ring that’s erythematous, and these are patients that were exposed to antibiotics. 04:07 Management: With minor, self-resolving, thank goodness. 04:12 SJS stands for Stevens-Johnson syndrome. 04:15 You may want to think of this as being erythema multiforme major. 04:20 TEN stands for toxic epidermal necrolysis. 04:24 Which one is more severe? TEN, they’re both severe, don’t get me wrong. 04:29 But which one involves a greater percentage of your skin, thus, increasing mortality? Toxic epidermal necrolysis. 04:37 Supportive care, and possibly, IVIG immunoglobulin. 04:44 Drugs that cause Stevens-Johnson syndrome and TEN. 04:47 Memorize these culprits, man. 04:50 Bactrim, the combination of trimethoprim and sulfamethoxazole. 04:55 Seizure medications: phenobarb, phenytoin. 04:58 Other antibiotics, and perhaps even, allopurinol. 05:00 These are some major drugs that you always want to keep in mind as a side effect, may result in Stevens-Johnson syndrome, and greater than 30% involvement of your skin, toxic epidermal necrolysis.
About the Lecture
The lecture Erythema Multiforme by Carlo Raj, MD is from the course Inflammatory Skin Diseases. It contains the following chapters:
- Erythema Multiforme
- Drugs That Cause SJS/TEN
Included Quiz Questions
A rash that develops after taking sulfa antibiotics, manifests with target lesions, and involves the skin and mucous membranes (i.e., at least two mucosal surfaces) affecting less than 30% of the body surface area is most suggestive of what disease?
- Stevens-Johnson syndrome
- Erythema multiforme
- Toxic epidermal necrolysis
- Erythema marginatum
- Erythema nodosum
What virus is most strongly associated with erythema multiforme minor?
- Herpes simplex virus
- Human papillomavirus
- Human immunodeficiency virus
- Hepatitis B
- Hepatitis C
Which of the following is the most appropriate management for patients with Stevens-Johnson syndrome?
- Supportive care
- Intravenous antibiotics
- Intravenous steroids
- Hemodialysis
- Methotrexate
Author of lecture Erythema Multiforme

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
the lecture was easy to understand and well done. i am feeling satisfied after listening to this lecture.
