Playlist
Show Playlist
Hide Playlist
Endometrial Adenocarcinoma


-
Slides Uterus Female Repro.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
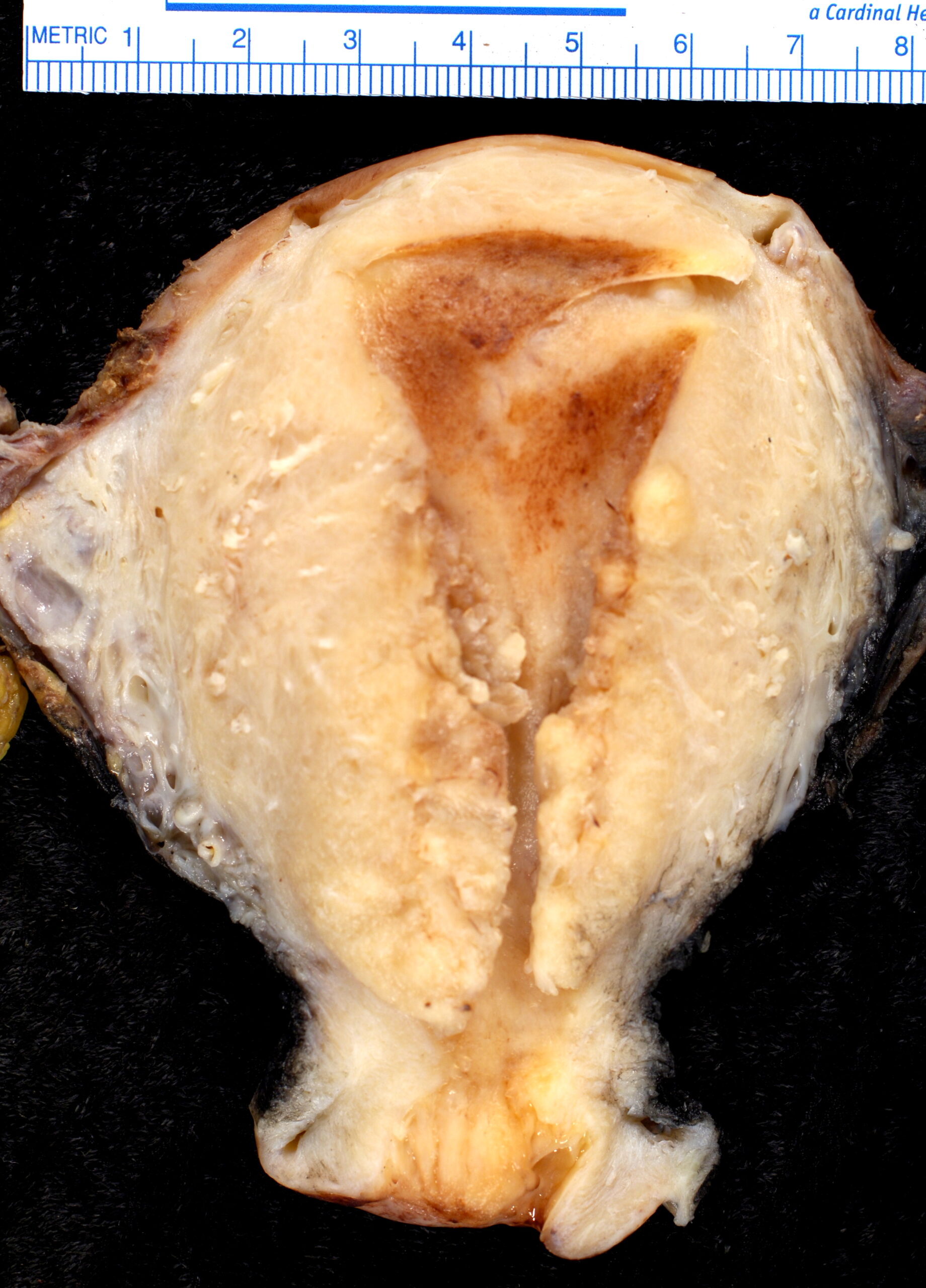
00:01 Our topic now, brings us into endometrial adenocarcinoma. 00:05 At this point, I’m hoping by you looking at this picture and that area that you see here in which it’s circular, the cells that are surrounding the circular area are lined by what’s known as your columnar glandular cells. 00:20 And you find this to be, well, increased in number, increased, increased glandular cells. 00:26 While here we have endometrial adenocarcinoma, it is the most common invasive cancer of the female genital tract. 00:31 Yes, that’s true if your patient may be coming from a developed country. 00:36 If however she’s coming from a developing country, then you’re thinking more along the lines of cervical invasive cancer and that is something that we already pointed out. 00:45 Here as well, as I told you earlier, with endometrial adenocarcinoma, you want to group this together with hyperplasia and the reason for that is the risk factors will be relatively similar. 00:57 Lots of estrogen exposure and symptoms here once again, you’re looking for bleeding that’s taking place in a female postmenopausal from the cervical os. 01:08 Uncommon in women younger than age 40. 01:11 That’s important for you to know. 01:13 As I said, post menopausal. 01:16 The risk factors for adenocarcinoma. 01:18 Here once again, estrogen exposure, obesity, infertility, lots of estrogen. 01:24 Endometrioid Endometrial Adenocarcinoma is the most prevalent form of endometrial carcinoma, accounting for 80% to 85% of all cases. This particular cancer is characterized by a sequence of genetic changes. 01:41 Specifically, alterations occur in tumor suppressor genes and oncogenes, which are critical in the regulation of cell growth. 01:50 When these genes are mutated, it can lead to uncontrolled cell proliferation, which is a hallmark of cancer development. 01:58 Initially, the cancer may present as a polypoid mass, which is a growth that protrudes from the lining of the uterus. 02:05 Alternatively, it may diffusely involve the endometrial lining, spreading across the surface. As the cancer advances, it can invade the myometrium.. From there, it has the potential to spread further to adjacent structures and regional lymph nodes. 02:23 In the later stages of the disease, cancer cells may travel through the bloodstream or lymphatic system and establish metastases in the lungs, liver, or bones. 02:34 Histologic grading is a key factor in diagnosis and treatment planning. 02:39 This grading is based on how much the cancer cells resemble normal cells under a microscope. Grade 1 tumors have well-formed glands and are considered the least aggressive. 02:49 In Grade 2 tumors, there's a mix of glandular structures and solid sheets of cells, with the latter comprising less than 50% of the tumor. 03:00 Grade 3 tumors, which are the most aggressive, are characterized by more than 50% of the tumor being made up of solid growth patterns. 03:08 These grades give us insight into the tumor's behavior and help guide the clinical approach to treatment. 03:13 The first image shown at the right is a gross anatomical photograph of a uterus that has been opened with a bivalve cut. 03:22 We can clearly see the interior of the uterus, with tumor growing on both the anterior and posterior walls. 03:28 Most of the tumor is present on the anterior wall. 03:31 It is irregular and hemorrhagic, contrasting sharply with the surrounding uninvolved tan-colored endometrial mucosa which has a smooth uniform appearance. 03:41 The tumor shows obvious invasion into the myometrium on the right side of the uterus —seen at the top of the picture as irregular solid areas with the myometrium. 03:52 Below this gross image, there is a high-power microscopic view of the tumor, stained with hematoxylin and eosin, which shows crowded back-to-back glands and areas of solid sheets of cells, which comprise less than 50 percent of the tumor, thereby classifying it as histologic Grade 2. 04:12 The cancer cells are subsets. 04:15 The subset of patients usually older develop what’s known as high-grade papillary serous carcinoma without a background of hyperplasia and that’s extremely dangerous. 04:25 So here, you kind of have a patient that goes onto endometrial cancer without any predisposing factor. 04:31 Scary. 04:32 It would be nice at least if there was some type of warning and maybe there was hyperplasia, nuclear atypia, and then at that point at least, you could take it -- I mean here also you’d be taking out the uterus, but at least you won’t have to worry about cancer per se. 04:44 So without a background of hyperplasia, a papillary high-grade serous, at least know this. 04:51 These exhibit what’s known as microsatellite instability and P53 mutation. 04:57 The last time we talked about microsatellite instability was dealing with what was known as HNPCC. 05:03 Hereditary nonpolyposis colorectal cancer. 05:06 And during that time, I mentioned what microsatellite instability was and I also mentioned MLH1 and MSH2. 05:13 Please do not forget, at least know one subset or one type of endometrial cancer known as your papillary serous in which a background or predisposing hyperplasia was not discovered.
About the Lecture
The lecture Endometrial Adenocarcinoma by Carlo Raj, MD is from the course Uterine and Fallopian Tube Disease.
Included Quiz Questions
Which of the following statements on the incidence of endometrial adenocarcinoma is TRUE?
- It is the most common invasive cancer of the female genital tract in developed countries.
- It is the least common invasive cancer of the female genital tract in developed countries.
- It is less common than leiomyosarcoma worldwide.
- It is less common than sarcoma botyroides in females older than 40 years.
- It is more common than cervical carcinoma in developing countries.
Which of the following statements regarding papillary serous carcinoma is FALSE?
- It usually occurs after a few months of developing endometrial hyperplasia.
- The patient population is usually older.
- It occurs without a background of endometrial hyperplasia.
- The cancer cells exhibit microsatellite instability.
- p53 mutations are present in the cancer cells.
Author of lecture Endometrial Adenocarcinoma

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
