Playlist
Show Playlist
Hide Playlist
Donovanosis (Granuloma Inguinale)

-
Slides Donovanosis InfectiousDiseases.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
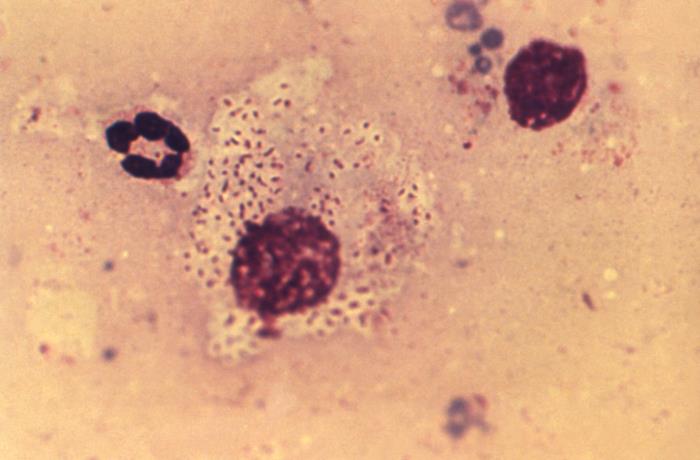
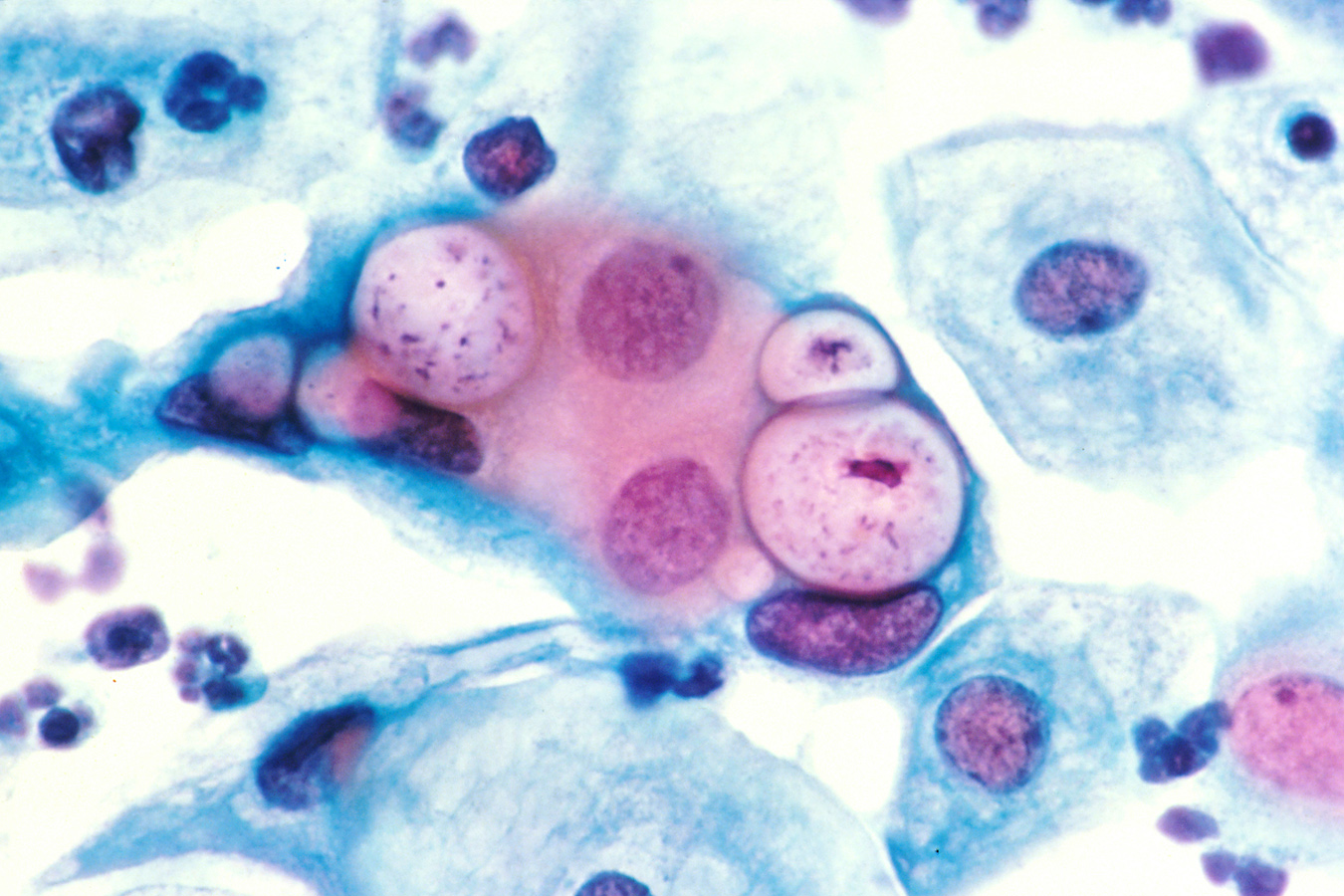
00:01 Continuing now with our discussion of sexually transmitted infections, we’ve come to donovanosis, also known as granuloma inguinale. 00:11 This is a sexually transmitted infection characterized by chronic ulcers, usually of the genital region and caused by an organism known as Klebsiella granulomatis. 00:25 Donovanosis is a relatively rare disease in the United States, with fewer than a hundred cases per year reported. 00:33 But it is endemic in the tropics – parts of India, the Caribbean, and parts of South America. 00:42 And it’s usually assumed to be sexually transmitted – sometimes, that’s harder to prove. 00:49 It’s more common in uncircumcised men for reasons that are not clearly understood. 00:58 It is not highly contagious probably accounting for the relatively few cases. 01:05 And there is some evidence that it can be transmitted non-sexually because there are persons who have extragenital lesions and it may be spread congenitally. 01:18 Granuloma inguinale is the old name for this disorder. 01:25 And because of confusion with the name lymphogranuloma veneruem, the name that’s now preferred for this disorder is donovanosis. 01:37 The cause, as I’ve mentioned, is Klebsiella granulomatis, and even that name has been changed. 01:45 That was formerly known as Calymmatobacterium granulomatis. 01:49 But DNA studies showed that it was actually related genetically to Klebsiella. 01:56 What this organism is it’s an encapsulated kind of pleomorphic Gram-negative rod, which you find in cytoplasmic vacuoles of large mononuclear cells. 02:08 What you see are bipolar densities, which give the appearance of a closed safety pin. 02:15 We call those Donovan bodies. 02:18 So when it’s sexually transmitted, it’s from intimate contact – genital-to-genital. 02:28 And like some of the other infections we’ve mentioned, starts out as a papule, which then becomes an ulcer, which then spreads to the lymphatics and the regional lymph nodes, and results in often very impressive widespread ulcers. 02:45 So not so much in the way of fluctuant lymph nodes, but it’s an ulcerative disease. 02:54 The incubation period is quite variable from 1 to a year after exposure. 03:02 The average is about 50 days after exposure to an infected person. 03:07 And this papule, or firm nodule, rapidly becomes ulcerative. 03:15 And you find these ulcers on the distal penis, the prepuce, coronal sulcus, and the penile shaft. 03:22 And in women, you find it in the labia minora, fourchette, the cervix, or even the anus. 03:31 The ulcer is pretty characteristic. 03:34 It has sort of a beefy red appearance and you would think this would be tremendously tender, but it’s really not. 03:42 It tends to have rolled edges, which bleed relatively easily. 03:47 One ulcer could coalesce to form a larger ulcer. 03:53 Unless this is treated, we can expect severe genital disfigurement, even pseudo elephantiasis, and the organism can disseminate to the liver and the bone. 04:08 Now to diagnose it, we simply need a microscope. 04:14 And so, direct microscopy of a smear from an ulcer and look for these Donovan bodies – I’m showing you one here – and you need some kind of a cell stain, and that cell stain would be the Giemsa, Wright, or a silver stain. 04:34 Now a Gram stain wouldn’t show you the attacked cell. 04:39 That’s the problem of the Gram stain because you heat-fix the Gram stain. 04:43 But with these cell stains, you use to fix them with methanol or some other fixative where you don’t distort the cell architecture, so you can see these organisms inside this Donovan body. 04:59 Culture of this organism is very difficult and not usually done. 05:05 And there are molecular techniques that are promising, but none that are ready for primetime. 05:12 And of interest, serology has essentially no role in the diagnosis of donovanosis. 05:21 The therapy of choice is either 1 gram of azithromycin once weekly for 3 weeks, or 500 milligrams daily for 3 weeks. 05:35 But notice we’re talking about prolonged therapy – doxycycline, ciprofloxacin, erythromycin, TMP/SMX, and even ceftriaxone. 05:49 And the reason that we want to treat for such a long time is we want to allow time for the ulcer to re-epithelialize and there may be still living organisms in an ulcer that has not completely closed over. 06:08 When you use ceftriaxone, either intramuscularly or intravenously, we’re not essentially sure of the duration, but prolonged therapy is usually recommended. 06:23 The expected outcome is progression of the ulceration if you don’t treat, but resolution of the ulcer if you do treat. 06:37 And it usually heals inward from the ulcer margins, so you can expect the re-epithelialization coming this way. 06:45 Partner management is problematic because of the prolonged incubation of this organism. 06:54 So you’re never sure if you treat it for 3 weeks – the partner – whether that is going to eradicate the incubating disease. 07:02 Furthermore, infection is actually rare in partners. 07:08 The CDC recommends that you screen all partners within 60 days prior to the symptom onset, but no further recommendations have been forthcoming. 07:20 And that concludes my discussion of donovanosis.
About the Lecture
The lecture Donovanosis (Granuloma Inguinale) by John Fisher, MD is from the course Genital and Sexually Transmitted Infections. It contains the following chapters:
- Donovanosis – Granuloma Inguinale
- Donovanosis – Signs/Symptoms
- Donovanosis – Management
Included Quiz Questions
Which best describes the characteristics of donovanosis lesions?
- Large non-tender beefy red ulcer with rolled edges that bleeds easily
- Multiple papules along the genital mucosa
- Itchy vesicular rash on the external genitalia
- Small well-demarcated tender ulcers with necrotic bases
- Circumscribed tender ulcers
The diagnosis of donovanosis is most commonly confirmed by which of the following techniques?
- Direct microscopy
- Sonography
- Culture
- Serology
- Nucleic acid amplification
Which of the following is a major complication of donovanosis?
- Extragenital extension
- Formation of a fluctuant buboes
- Inguinal abscesses
- Elephantiasis
- Toxic shock syndrome
A 28-year-old woman from the Caribbean presents with beefy red ulcers along the labia minora. Physical examination shows non-tender bleeding ulcers. Inguinal lymphadenopathy is absent. Direct microscopy of a smear from the ulcers shows rod-shaped organisms in the cytoplasm of mononuclear phagocytes. Which of the following is the most likely pathogen?
- Klebsiella granulomatis
- Neisseria gonorrhoeae
- Chlamydia trachomatis
- Treponema pallidum
- Herpes simplex virus
Which of the following is the most appropriate management of donovanosis (granuloma inguinale)?
- Appropriate wound care and at least three weeks of systemic antibiotic therapy
- Appropriate wound care and topical antibiotic therapy
- A single antibiotic dose
- Hospitalization and ten days of intravenous antibiotics
- No therapy is required
Author of lecture Donovanosis (Granuloma Inguinale)

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
