Playlist
Show Playlist
Hide Playlist
Diverticulitis with Case

-
Slides Gastroenterology 08 Disorders Large Intestine I.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
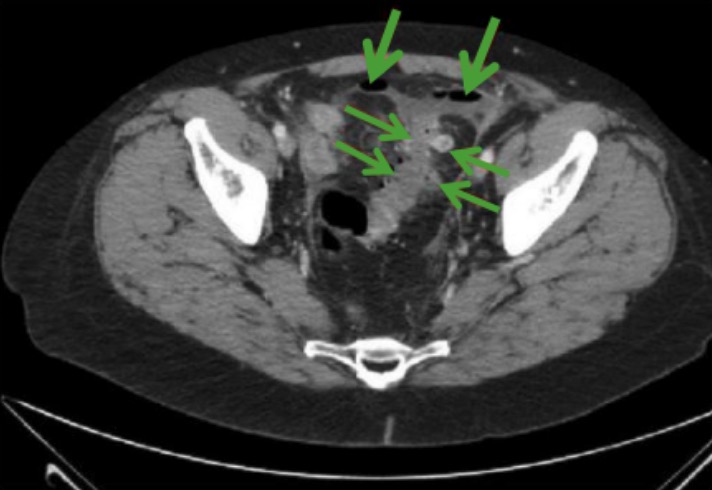
00:01 Welcome, today we'll be discussing disorders of the large intestine. 00:05 So we'll begin with a case. 00:07 We have a 68-year-old woman who presents to the ED with 3 days of abdominal pain in the left lower quadrant. 00:14 She has had subjective fevers and chills but no changes in her urination, bowel habits, nausea, vomiting or blood in her stool. 00:22 Her past medical history includes hyperlipidemia, and irritable bowel syndrome with chronic constipation. 00:28 Her vitals show a temperature of 38, heart rate of 100 and she appears to be in mild discomfort. 00:35 She has mild tenderness to palpation in the left lower quadrant without rebound or guarding. 00:41 Her labs are notable for a leukocyte count of 13,500. 00:46 And her complete metabolic panel and urinalysis is unremarkable. 00:50 What would be an appropriate next diagnostic step? So before we answer that, let's go through some key features of this case. 00:58 She has acute left lower quadrant abdominal pain with fevers and chills which would prompt you to consider an infectious cause. 01:06 She does have a history of chronic constipation and on exam, she's febrile, tachycardic, has leukocytosis with a potentially localizing sign of abdominal tenderness. 01:21 So we'll go through a very broad differential diagnosis for this patient. 01:26 If you were to see this patient presenting to you in the ED, you would first think about gastrointestinal causes. 01:33 Those may include diverticulitis, ischemic bowel, infectious colitis and other things listed here. 01:40 If we think anatomically now, moving on from the GI system, you also have to worry about the genitourinary system. 01:46 So things like cystitis and pyelonephritis can also present this way. 01:51 Because she's a woman, you should always have gynecological causes on your differential. 01:57 So a ruptured ovarian cyst or ovarian torsion could lead to her presentation. 02:03 You also must remember that there are large vascular structures in this area, so inflammation of the aorta or various blood vessels may lead to vasculitis. 02:12 She may also have aortic dissection. 02:16 and then, kind of the miscellaneous areas, she may have abscess in her abdominal wall, a hematoma, an abscess in her psoas muscle or hemorrhage into her retroperitoneal space. 02:30 So this is a very broad differential, so let's think critically through it and kind of narrow it a bit. 02:37 So, because she's coming in with left lower quadrant pain, you should always have diverticulitis at the top of your differential. 02:45 Moving on to the GU system, she doesn't have any particular symptoms of the genitourinary tract and her urinalysis is negative, so you can kind of cross these things off your differential. 02:57 Because she's a woman, you should always keep a ruptured ovarian cyst and ovarian torsion on your differential and rule them out. 03:05 And then consider that she may also have a psoas abscess since this may correspond with her anatomic location of pain. 03:12 All of the other causes listed here are possible but less likely based on the acute(ness) of her presentation and the location of her pain. 03:24 So now let's review some important definitions. 03:27 We mentioned diverticulitis earlier. 03:30 There are several different terms that we should go through first. 03:33 The first is "diverticulum". 03:35 So this is when you have just an asymptomatic outpouching in the colonic mucosa just due to weakness in the muscle wall. 03:43 "Diverticulosis" just refers to the presence of diverticula. 03:49 When we talk about "diverticulitis", that's when you have inflammation of a diverticulum. 03:57 So here you can see different types of diverticulum. 04:02 On the bottom right, this is an example of a regular diverticulum. 04:06 Above that, you see a ruptured diverticulum and to the left, you see an example of diverticulitis where the outpouching then gets obstructed and leads to inflammation. 04:18 So now let's go to some risk factors of diverticulitis. 04:22 Advanced age is the first risk factor as most cases occur after age 85. 04:27 This is because as we age, the muscle wall in our colon becomes weaker. 04:33 Patients who have a history of chronic constipation are also at risk for developing diverticulitis. 04:38 This is because with frequent straining for the passage of bowel movements, this can lead to weakness in the colonic wall. 04:46 People who have low dietary fiber or do not exercise much are also at risk. 04:52 Obesity is another risk factor. 04:54 And prior episode of diverticulitis puts you at risk for having more in your lifetime. 05:02 So acute diverticulitis is caused by a blocked diverticulum which then leads to a nice space where bacteria are able to proliferate and cause inflammation. 05:14 Patients will come in with abdominal pain, typically they'll note always in the left lower quadrant. 05:20 They may have fever and they may have a change in their bowel habits. 05:23 The diagnosis is mostly made based on clinical symptoms but if they have severe presentation, you should consider doing a CT imaging to look for any complications. 05:34 So here on the right, you see an example of a CT scan. 05:37 The horizontal areas are showing areas of perforated diverticulitis and the downward arrows at the top of the image show you several pockets of free air in the abdomen. 05:49 This is always a very concerning sign as this tells you that you have a perforated viscus or organ and in this case has resulted from a perforated diverticulum. 06:03 So treatment is by allowing bowel rest, you may put patients on a liquid diet. 06:09 You should cover for a colonic flora with antibiotics, so targeting gram negative and anaerobic bacteria. 06:17 And if you see any complications, you should consult surgery. 06:22 The mainstay of treatment however, is just prevention. 06:25 So counseling patients on a high fiber diet to make sure that they don't develop future episodes. 06:33 We spoke a bit about complications of diverticulitis. 06:36 There are several complications of which you should be concerned. 06:39 The first is an abscess. 06:41 This is when an area of infection perforates outside of the diverticulum and then becomes walled off. 06:49 You can see here several air-fluid levels that are indicative of an abscess on the CT scan. 06:57 The next common complication is a fistula. 07:01 So anytime you have inflammation of the colon, it can cause an abnormal connection or tracks to form between two structures. 07:09 Here in the CT scan, you see an example of a sigmoid diverticulitis and the area points to a fistulous tract leading to an abscess. 07:20 The last complication is the most dreaded of all, which is peritonitis. 07:25 This is when you just have perforation of the diverticulum into the free abdomen which leads to the development of free air and then inflammation of the peritoneal space. 07:35 Here on this CT scan, this is a very concerning finding. 07:38 You see a large amount of free air at the top of the abdomen which indicates that something has perforated. 07:47 So now we return to our case. 07:49 We have a 68-year-old woman who is having acute left lower quadrant abdominal pain with fevers and chills. 07:55 She does have a history of chronic constipation which puts her at risk for diverticulitis and her exam and vital signs are all consistent with this presentation. 08:06 So, the next appropriate step in diagnosis would be to perform a CT image of the abdomen to look for diverticulitis and its any complications.
About the Lecture
The lecture Diverticulitis with Case by Kelley Chuang, MD is from the course Disorders of the Small and Large Intestines.
Included Quiz Questions
Which of the following is the best diagnostic test for diverticulitis?
- Abdominal CT
- Colonoscopy
- Barium swallow
- Abdominal X-ray
- Sigmoidoscopy
Which of the following is a risk factor for diverticulitis?
- Constipation
- Younger age
- Anorexia
- High dietary fiber intake
- Diarrhea
Which of the following decreases the risk of diverticulitis?
- High-fiber diet
- Low-fiber diet
- Antibiotics
- Liquid diet
- No physical activity
Which of the following is not one of the complications of diverticulitis?
- Retroperitoneal hemorrhage
- Fistula
- Abscess
- Peritonitis
- Bowel blockage
Author of lecture Diverticulitis with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I would recommend to others in the workup of diverticulitis
