Playlist
Show Playlist
Hide Playlist
Disseminated Intravascular Coagulation (DIC) in Children

-
Slides DICITP Pediatrics.pdf
-
Download Lecture Overview
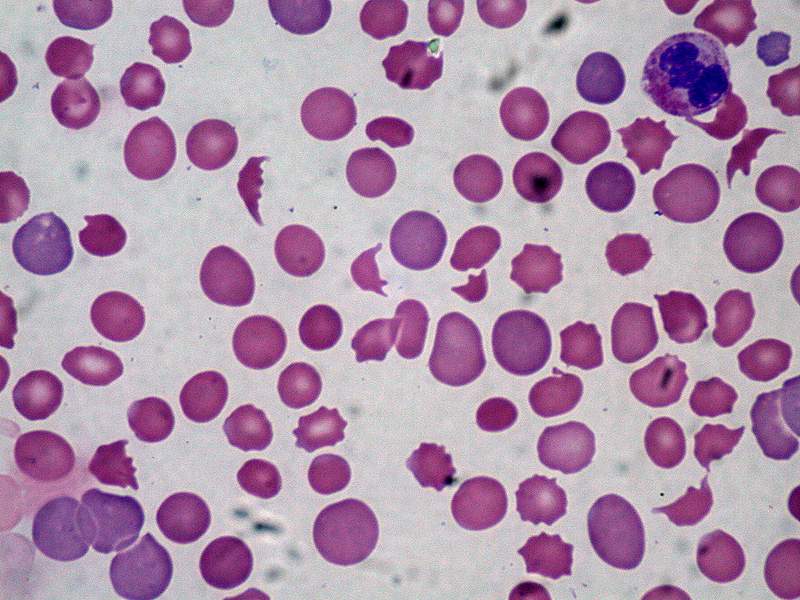
00:01 In this lecture, we’re going to discuss 2 major causes of acute hypercoagulability in an otherwise normal child. 00:08 One is DIC or disseminated intravascular coagulation and the other is ITP or immune thrombocytopenic purpura. 00:18 Let’s start with DIC. 00:20 So DIC is a systemic body wide activation of the coagulation cascade. 00:27 This can cause both microemboli but also an overall overconsumption of clotting factors, which then results in hemorrhage. 00:37 It can either be low grade or chronic or it can be acute and very severe. 00:43 So there are many causes of DIC. 00:46 It could just be surgery. 00:47 It could be a traumatic event. 00:49 It could be an overwhelming bacterial infection or it could be cancer. 00:53 The idea here is that it’s something that’s activating the clotting cascade. 00:59 One unusual cause of DIC that’s specific to children is Kasabach-Merritt syndrome. 01:05 All these infants you can see on this slide have hemangiomas and this can be large. 01:11 And in these infants, all of these infants, they develop Kasabach-Merritt syndrome. 01:15 Kasabach-Merritt is when there’s a consumption of these coagulable products inside the hemangioma. 01:23 Sometimes, these hemangiomas are on the outside of the body and sometimes they are on the inside of the body and it can be hard to figure out and very challenging to treat. 01:32 Another unusual specific to children is snake bites. 01:36 Of course adults get snake bites too, but the majority of snake victims are actually children who don’t know better than to avoid handling poisonous snakes. 01:47 Snake bites can cause a DIC picture and that’s typically the pit vipers rather than something like the coral snake which is more of a neurotoxin. 01:56 Also, patients may simply develop sepsis and we do see DIC sometimes especially in neonatal sepsis. 02:03 Okay. 02:04 What are the signs and symptoms of DIC? These patients will typically have acute and severe bleeding from the nose, from the mouth, from the orifices. 02:14 They will develop bruising and, body wide, they may have purpura and petechiae. 02:20 The blood may be oozing from IV sites or surgical sites and may be coming from the rectum. 02:25 They may start coughing up blood and have a pulmonary bleed or they may develop a stroke and have a CNS hemorrhage. 02:32 The bleeds may happen really anywhere and result in end-organ dysfunction. 02:37 This is a very severe disease. 02:40 So how do we make the diagnosis? There are several labs that can key us in to a diagnosis of DIC. 02:47 Patient should have a prolonged PT/PTT because they are having consumption of their clotting cascades, both intrinsic and extrinsic. 02:55 They may have decreased fibrinogen which is used to create clots, because in those areas where those clots are forming, the rest of the blood has less of it. 03:05 Likewise, they will have increased fibrin split products, a side effect of having clotting happening elsewhere in the body. 03:14 The D-dimer is very likely to be elevated in DIC. 03:19 In fact, it’s ubiquitous. 03:21 So what’s interesting about the D-dimer is if that’s normal, it’s almost convincing that your patient does not have DIC. 03:30 That said, there is a lot of false positive D-dimers. 03:33 The patient could simply have a bad viral illness, for example, and have an elevated D-dimer, but a D-dimer that’s normal assures you that this is not DIC. 03:42 In the CBC, we will notice low platelets as a result of consumption in those areas where there are clots. 03:49 Okay. 03:51 How do we manage it? Well, first we need to treat the underlying cause. 03:56 If it’s an infection, we need to give the antibiotics that are necessary to treat the infection, because otherwise this is just going to keep burning. 04:04 Next, we’re going to replace consumed products. 04:06 In particular, these patients may require platelets. 04:10 They may require fresh frozen plasma and they may require cryoprecipitate. 04:16 Basically, they need those factors back in their clotting cascade.
About the Lecture
The lecture Disseminated Intravascular Coagulation (DIC) in Children by Brian Alverson, MD is from the course Pediatric Hematology.
Included Quiz Questions
Which of the following lab findings is most consistent with disseminated intravascular coagulation?
- Increased D-dimer
- Thrombocytosis
- Decreased fibrin split products
- Increased fibrinogen
- Conjugated hyperbilirubinemia
Which of the following clinical findings in sepsis is less specific for disseminated intravascular coagulation?
- Hypertension
- Bleeding from IV sites
- Bruising and purpura
- Rectal or GI bleeding
- Pulmonary or CNS bleeding
Which of the following is contraindicated in a patient with disseminated intravascular coagulation?
- Coumadin
- Platelets
- Cryoprecipitate
- Fresh frozen plasma
- Antibiotics
Author of lecture Disseminated Intravascular Coagulation (DIC) in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
2 customer reviews without text
2 user review without text
