Playlist
Show Playlist
Hide Playlist
Differentiating Seizure from Syncope and from Psychogenic Nonepileptic Spells (PNES)

-
Slides Seizures Epilepsy Approach to a New Spell.pdf
-
Download Lecture Overview
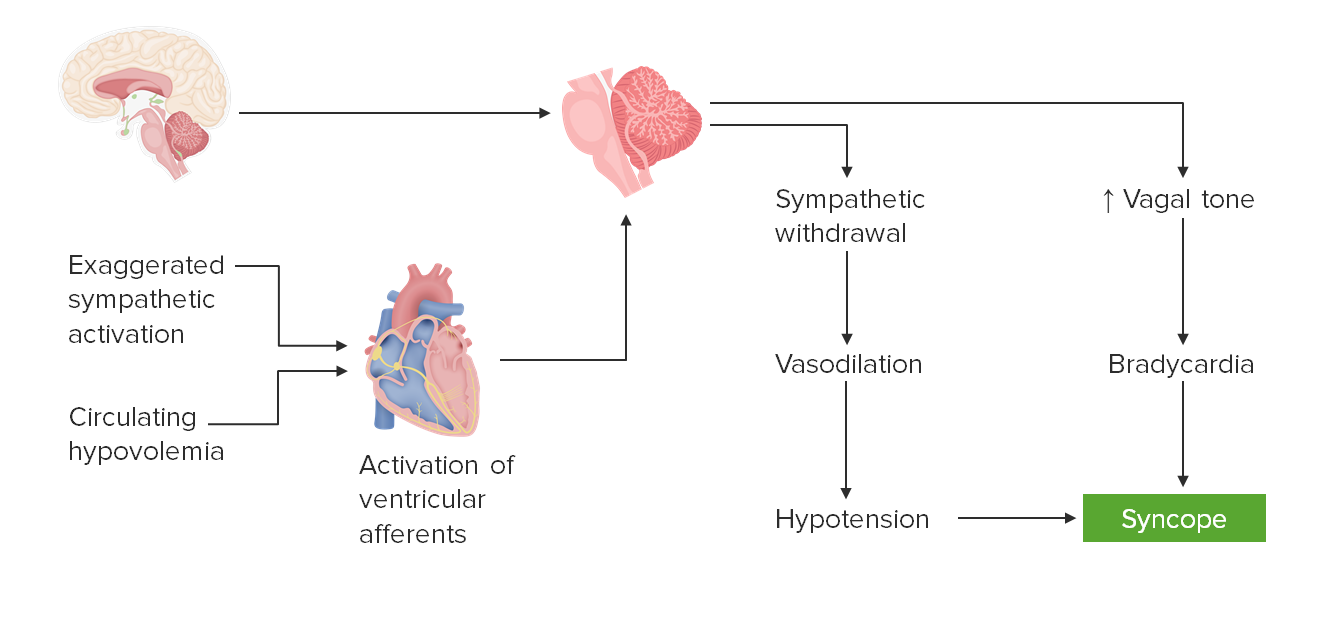
00:01 When thinking about how to differentiate seizures from other common mimics, other common differential conditions, one is syncope and in this case we needed to differentiate seizure from syncope, and there are some features we can use to differentiate between these two conditions. 00:17 The first is the position in which they occur. 00:19 Seizures occur in any position, syncope typically occurs, when patients are standing upright from a seated or lying position. 00:26 The duration of a seizure is often one to two minutes, about 90 to 95% of seizures will resolve spontaneously within the first three minutes. 00:34 Syncope is much shorter, lasting only 30 seconds or so when the patient is has lost consciousness or have altered awareness. 00:43 The tonic-clonic phase is present in many motor seizures. 00:47 We can see that with syncope as well with convulsive syncope, but again, it's often very short with a couple of jerks or a couple of shakes throughout the body after the patient has passed out. 00:59 Incontinence is common in patients with generalized-tonic clonic seizures, but quite rare and syncope. 01:04 And postictal amnesia is often present, sometimes prolonged and seizures lasting 15 minutes up to two hours on average, but it's very rare and would be exceptional to see in syncope patients come right back to after a convulsive syncope event. 01:23 Some other features of convulsive syncope that point us in that direction and some were present in this case, we look for triggers like orthostasis, changing of posture, or history of cardiac arrhythmia's, dehydration or an emotional stress can precipitate syncope. 01:37 Anxiety, pain, hyperventilation, and coughing and micturition can be associated with situational syncope. 01:44 We also think about the pre-episode description, convulsive syncope should lack an aura that's frequently present in focal-onset epilepsy. 01:52 We also interrogate and investigate the episode. 01:55 Convulsive syncope begins with syncope and ends with a convulsion. 02:00 There typically is no tongue biting, and for seizures we often see lateral tongue biting, but often don't see tongue biting and convulsive syncope, and incontinence is rare. 02:10 After the event, there is a rapid return to baseline and really lacking post event or postictal confusion. 02:18 Events are features that would favour epileptic seizures include an aura, the brief duration of convulsions lasting one to two minutes longer than convulsive syncope, postictal confusion, abnormal posturing that is stereotyped the same thing with each event, amnesia to the event and continence during the event. 02:36 Events that arise from sleep. 02:38 Convulsive syncope would be very exceptional, quite rare to occur out of sleep and seizures can occur from sleep. 02:44 Self-injury, lateral tongue biting, and eyes opening at the onset of the event would favour seizures as opposed to convulsive syncope. 02:52 So some of these things can help us in evaluating this patient and certainly were helpful in our case. 02:58 How do we differentiate seizures from psychogenic non-epileptic spells, functional spells, these have many names, behavioral, non-epileptic events, and a number of other names have been used to describe, these we'll call them PNES or psychogenic non-epileptic spells. 03:15 Again, if we think about the position, seizures can happen at any position. 03:19 Whether the patient is standing or lying or seated. 03:22 Psychogenic non-epileptic spells typically happen when the patient is lying down and safe. 03:27 The time and place, seizures can happen day or night. 03:30 Psychogenic non-epileptic spells are quite uncommon at night and they usually occur in the daytime. 03:37 The duration of seizures is typically very short resolving within one to two to three minutes. 03:42 Psychogenic non-epileptic spells are often less than two minutes, but sometimes can be quite prolonged. 03:47 Motor activity is common in seizures. 03:50 With psychogenic non epileptic spells, it's less common in varying motor activity as described during the events. 03:56 Postictal amnesia is usually prolonged with seizures, and quite short with psychogenic non-epileptic spells. 04:03 And importantly, the eyes are typically open during a seizure. 04:06 Patients don't close their eyes often opened with a staring trance like appearance, this distant stare. 04:14 With psychogenic non epileptic spells, we often see the eyes are closed and patients may even have forced eye closure that is resisted with eye opening. 04:23 In fact, we can use this nice mnemonic bad spells to think about some of the features of psychogenic non-epileptic spells that help us to differentiate between these two disorders. 04:32 The B is breathing, post event or post convulsion breathing is typically normal or fast. 04:38 In psychogenic non epileptic spells, which is different from seizures where patients may bright or phrenic. 04:43 Abrupt cessation is a feature of psychogenic non-epileptic spells distractibility, side to side head movement or limb shaking, pelvic thrusting, eyes and mouth shut tight. 04:55 That's a really important finding that we asked both patients and other observers. 05:00 Lack of stereotyped behavior. 05:03 Stereotypic events should raise the suspicion for seizure in psychogenic non-epileptic spells often lack that stereotypic nature. 05:11 The spells are different from spell to spell or event to event and the semiology what happens first, second, third, throughout the event may change for a psychogenic non-epileptic spell, which is a typical for seizures. 05:24 And psychogenic non-epileptic spells often stop and go. 05:27 They can stop and start and stop and start during the episode which would raise our suspicion for this diagnosis. 05:33 Some other features we see rocking and thrashing or side to side movements, pelvic thrusting, should raise suspicion for this aetiology. 05:40 We can see bizarre behavior which can be difficult to differentiate between frontal lobe epilepsy and PNES, but should raise suspicion. 05:50 Vocalizations with emotional content, out of phase of the extremity movements would suggest us psychogenic non-epileptic diagnosis. 05:59 And again, some other key events that can suggest a diagnosis of psychogenic non-epileptic seizures would be non traditional triggers, events that occur in the waiting room of a clinic or hospital. 06:12 Histrionic behavior during the examination, rapid cognitive postictal recovery, ability to induce a seizure and presence of other conditions like fibromyalgia chronic pain or chronic fatigue syndrome, which can co occur with psychogenic non-epileptic spells.
About the Lecture
The lecture Differentiating Seizure from Syncope and from Psychogenic Nonepileptic Spells (PNES) by Roy Strowd, MD is from the course Seizures and Epilepsy.
Included Quiz Questions
Which statement is the most accurate with respect to seizures?
- An aura is more common during a seizure than during a syncopal episode.
- Seizures have a shorter duration than a syncopal episode.
- A patient’s eyes are typically closed during a seizure.
- Patients rapidly return to their baseline after a seizure.
- Patients rarely experience incontinence during a seizure.
Which statement is most accurate when discussing convulsive syncope?
- Loss of consciousness occurs prior to convulsions.
- Patients are typically amnestic to the event.
- Patients typically experience an aura.
- Patients experience a prolonged return to baseline.
- Episodes typically occur while patients are lying down.
Which statement is most accurate when discussing Psychogenic Nonepileptic Spells?
- A side-to-side pattern of head shake is common.
- PNES typically occur when a patient is upright.
- The patient’s eyes are usually open throughout the episode.
- Patients experience a prolonged return to baseline after the episode.
- PNES usually occur at night.
Author of lecture Differentiating Seizure from Syncope and from Psychogenic Nonepileptic Spells (PNES)

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
