Playlist
Show Playlist
Hide Playlist
Differential Diagnoses – Hyperthyroidism (Thyrotoxicosis)

-
Slides Hyperthyroidism incl. Graves Disease.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
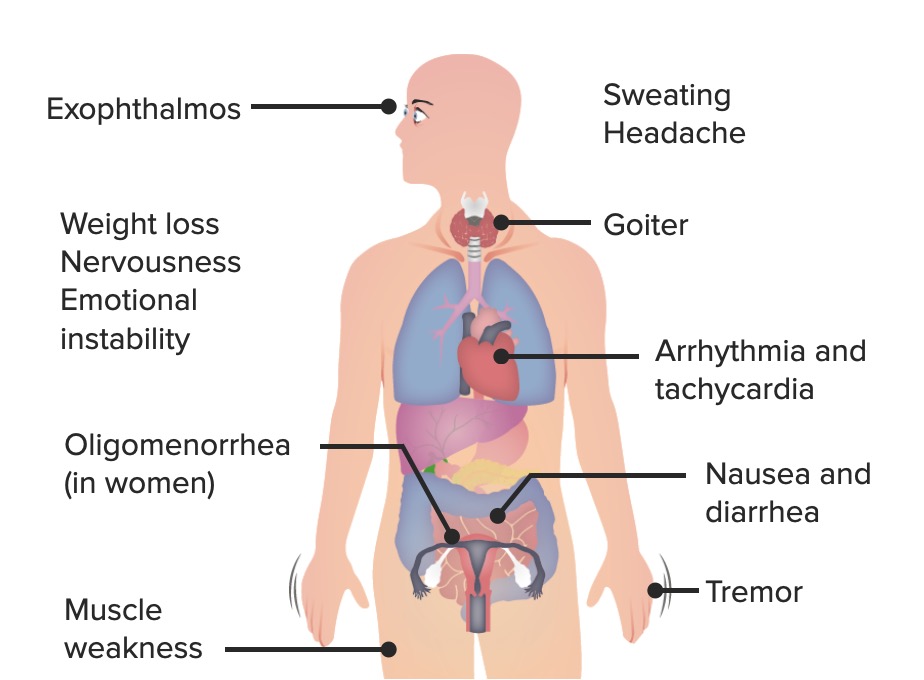
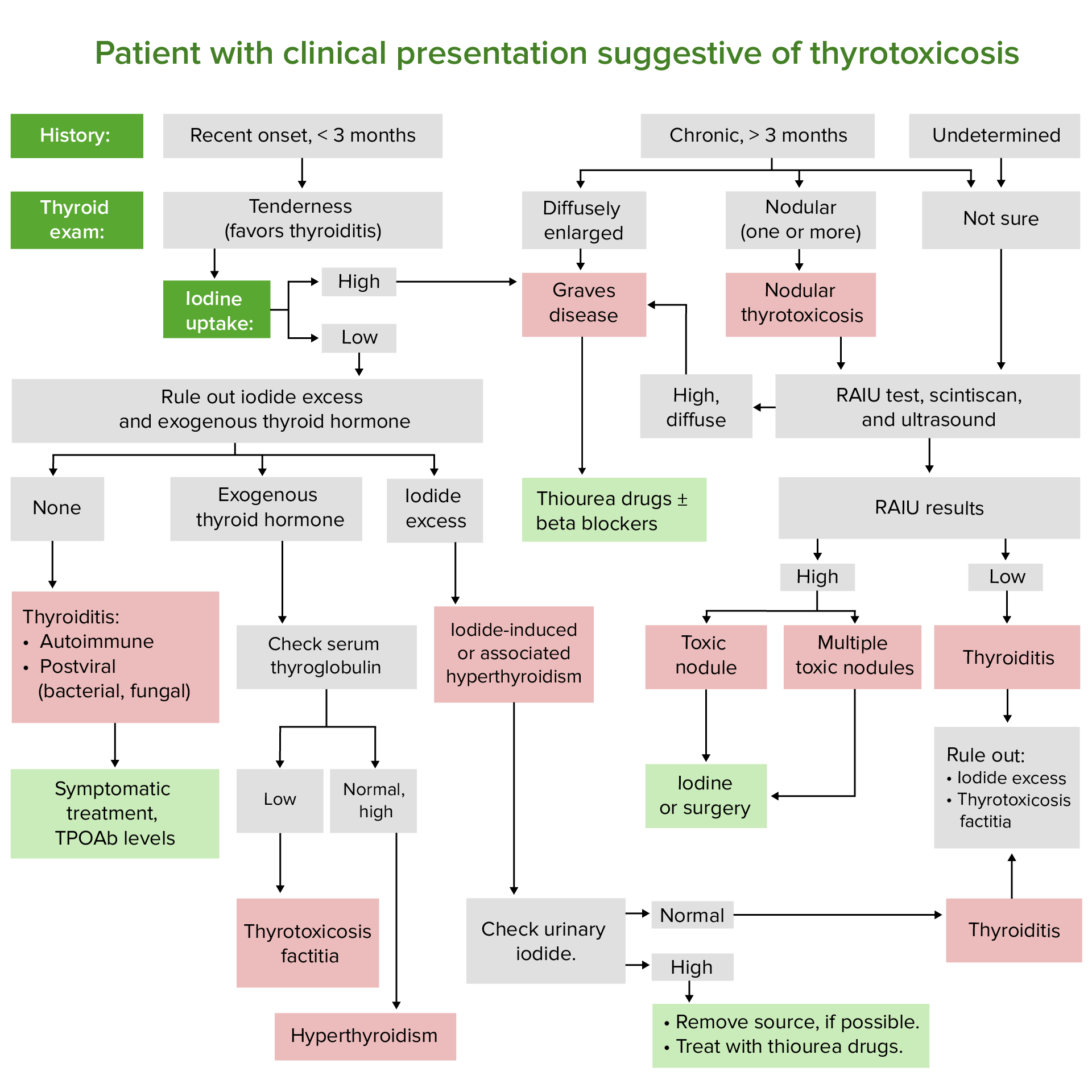
00:01 On this table, we’ll take a look at differentials of your hyperthyroidism. 00:05 Pretty much repetitive of the algorithm that we saw earlier, however, this time in a table format. 00:10 However you wish to learn, make sure that you know these important differentials. 00:14 We’ll divide this into the following columns and I’ll walk you through this: causes, mechanism, thyroid exam and the radioactive iodine and initially, it will be hyperthyroidism with a normal or high radioactive iodine uptake. 00:30 First, autoimmune thyroid diseases will be our-our organization or our first category. 00:36 Hashitoxicosis, what does that mean? Remember, with Hashimoto, I think we’re clear now that initially there is every possibility with that lymphocytic infiltration of the thyroid gland in which your colloid is being destroyed in releasing T3,T4 presenting how? Initially, with hyperthyroidism. 00:54 That’s my topic for this entire table. 00:57 This is then called Hashitoxicosis, how appropriate? Initially, you are going to have those autoimmune or antibodies that are then attacking maybe the thyroid globulin or maybe it is then attacking the peroxidase, those are the most common ones. 01:12 It could really have destruction anywhere. 01:15 Thyroid exam, you’re going to feel a goiter and here, initially, you’re going to find increased radioactive iodine uptake. 01:23 In Graves’ disease, this is your TSI that we talked about plenty of a diffused goiter and here it will be a diffused radioactive iodine uptake. 01:34 If you take a look at a scintigram here, take a look at the thyroid gland and you see these two lobes that are “lit up” quote and quote that’s because the entire thyroid gland diffusely is taking up radioactive iodine uptake or radioactive iodine. 01:51 The second organization will be autonomous thyroid tissue. 01:55 Uptake may be a low, if recent iodine load led to iodine induced hyperthyroidism. 02:00 Let’s take a look. 02:01 We have toxic multinodular goiter, toxic adenoma… who is your patient? Elderly. 02:06 Remember that picture that I showed you where you had a diffused enlargement of the neck? The thyroid gland was huge with lots of cysts and with such enlargement of the thyroid gland, there is every possibility that you may then rupture blood vessels and therefore cause haemorrhage into the cysts. 02:25 Activating gene mutations, nodules is what you’re going to find. 02:31 Thyroid exam usually greater than two and a half centimetres. 02:35 Here, the type of uptake, not diffused but focal. 02:39 Each nodule behaves like increased activity. 02:44 Choriocarcinoma a trophoblastic disease and we have hyperemesis gravidarum. 02:49 Here, you find hCG which behaves like TSH, minimal goiter, but you’re going to find an increase in radioactive iodine. 02:58 Then we have pituitary tumour with increased TSH, minimal goiter, increased radioactive iodine… welcome to secondary hyperthyroidism. 03:07 Next, we’ll take a look at hyperthyroidism with near absent radioactive iodine uptake, what does this take us into in terms of category? Differentials will be thyroiditis including painful, painless, postpartum, radiation thyroiditis. 03:24 The thyroid glands are being destroyed the patient is now presenting how? Hyperthyroidism. 03:31 Destruction releases of your stored hormones; tender and sub-acute, what does sub-acute mean to you? Viral, non-tender in silent. 03:40 Here, the thyroid gland is being destroyed, you cannot expect your thyroid gland to take up the radioactive iodine. 03:48 Iodine induced here iodine surplus called Jod-Basedow, with iodine surplus here the thyroid gland says, “I’m producing enough T3, T4… why would I want to produce more?” Nodular diffused goiter, decreased radioactive iodine. 04:06 Struma ovarii, we talked about, we have metastatic follicular thyroid cancer, that’s a big one. 04:12 This is ectopic thyroid tissue and we have normal thyroid exam. 04:18 Here, once again, radioactive iodine is decreased over the thyroid… over the thyroid. 04:25 What do you mean? Huh, what if you find an ovary that behaves like a thyroid gland? That’s Struma ovarii, a derivative of teratoma. 04:39 There it would be taking up iodine, do you understand the significance when it says radioactive iodine uptake over the thyroid? There it will be depressed. 04:47 But, if it’s located ectopically either metastatic and follicular, especially enough to metastasize; the follicular type of thyroid cancel off the metastasize. 04:57 That is not the most common though; what is common is papillary. 05:00 And we have exogenous and factitious. 05:03 You’re taking up T3 and T4, you’re going to knock out or you’re going to create negative feedback with decreased TSH, decreased receptor activity, radioactive iodine is depressed. 05:14 Ladies and gentlemen, once you fully have understood the foundation of hyperthyroidism initially and prior to this, the physiology, you go through the algorithm and you go through tables, there is absolutely no way that you could possibly miss any question. 05:30 You have yourself a proper educated guess.
About the Lecture
The lecture Differential Diagnoses – Hyperthyroidism (Thyrotoxicosis) by Carlo Raj, MD is from the course Thyroid Gland Disorders.
Included Quiz Questions
What is NOT a characteristic of Hashitoxicosis?
- Activating gene mutation
- Presents anti-thyroid antibodies
- Goiter
- Hyperthyroidism
- Decreased RAIU
On the RAIU scan, increased nodular uptake is present. The patient is elderly and is complaining of anterior neck swelling. Palpation reveals the presence of nodules. What is the most likely diagnosis?
- Toxic multinodular goiter
- Pituitary adenoma
- Graves' disease
- Hashitoxicosis
- Choriocarcinoma
What is the pathophysiology of hyperthyroidism in hyperemesis gravidarum?
- Increased hCG stimulates the thyroid gland.
- TSI
- Anti-thyroid antibodies
- Increased TSH
- Activating gene mutation
Author of lecture Differential Diagnoses – Hyperthyroidism (Thyrotoxicosis)

Carlo Raj, MD
Customer reviews
3,5 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
This is a really good overview of the previous discussions. The small mistake about radio-iodine uptake is Hashitoxicosis should be fixed, but the rest is pretty great.
Good table but a discussion of subsequent investigations to further characterise the nodule is warranted. For example following up a cold nodule with U/S guided FNA . The algorithm wasn't took clear for example starting with thyroid function test, followed by iodine uptake and further imaging/biopsy
