Playlist
Show Playlist
Hide Playlist
Development of Tongue and Thyroid Gland

-
Slides 04-17 Development of Tongue and Thyroid Gland.pdf
-
Reference List Embryology.pdf
-
Download Lecture Overview
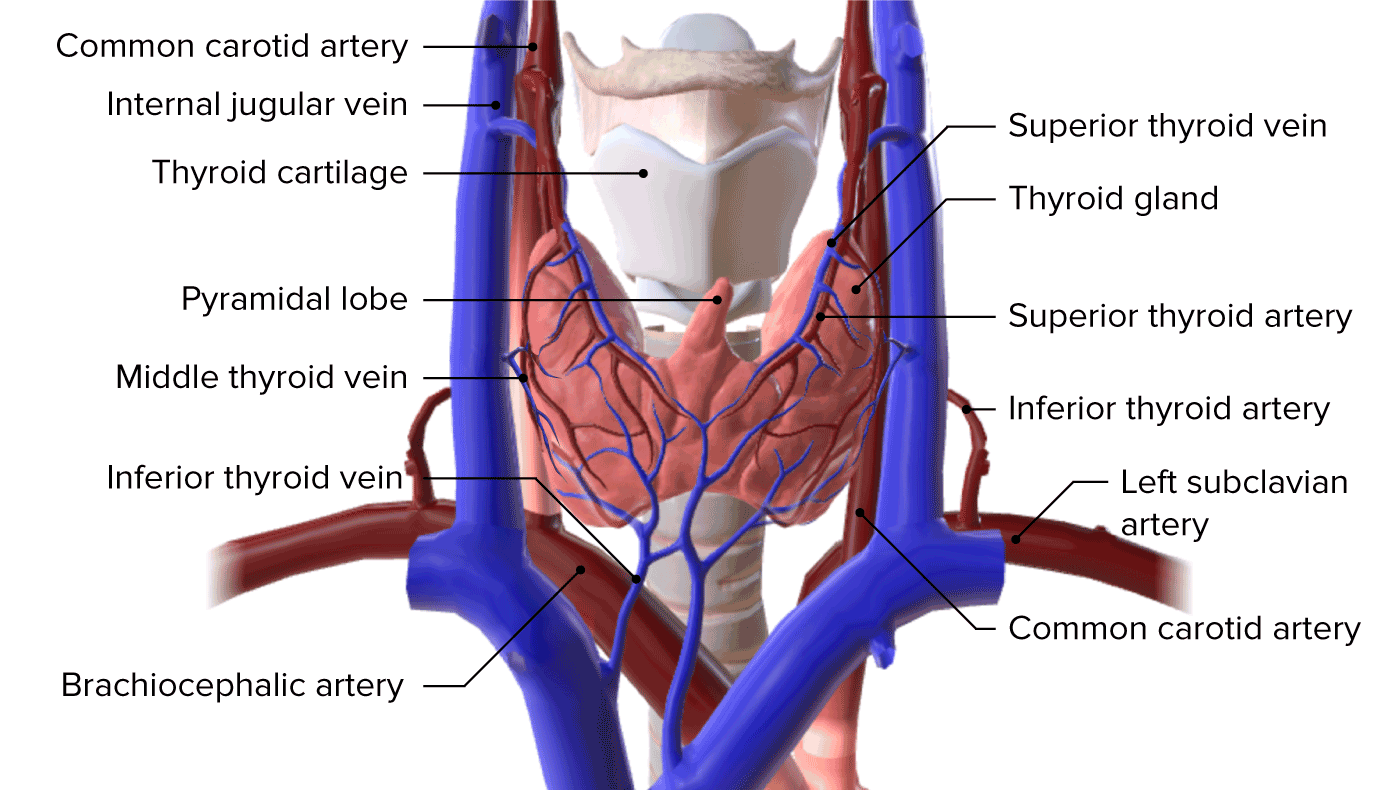
00:01 Hello. We´re now gonna discuss the development of the tongue and the thyroid gland. 00:06 Believe it or not, these two structures are actually intimately related even though they don´t appear to be very close to each other when we look at their normal confirmation in an adult. 00:14 Now, the primitive mouth called the stomodeum is going to open into the gut tube. 00:20 Now, the initial first portion of it is called the pharynx and it´s the inside of the pharyngeal arches that we´ve discussed previously. 00:27 So the pharyngeal arches internally are lined by endoderm and this endoderm has covering of the pharyngeal arches as well as the little spaces in between adjacent pharyngeal arches. 00:40 Now, in addition to the pharyngeal arches, something truly strange happens. 00:45 The somites from the occipital region migrate along the floor of the pharynx, the floor of those pharyngeal arches, and migrate forward to actually form swellings in the very front part of the stomodeum. 00:58 As they do so, they´re going to drag along their innervation cranial nerve number 12, the hypoglossal nerve. 01:04 Now, as the somites from the occipital region migrate underneath the mucosa of the pharyngeal arches, they´re going to create two lingual swellings on either side. 01:14 The lateral lingual swellings and one right in the midline, the median lingual swelling. 01:19 These are going to be located just underneath the mucosa of the first arch. 01:23 Just posterior to that is a small swelling under the second arch. 01:27 This is called the copula and the third and fourth arch have what´s referred to the hypopharyngeal eminence underneath their mucosa. 01:36 These are all derived from the occipital somites and as they move, they´re dragging their innervation behind them and that´s going to be once again cranial nerve 12. 01:47 Now, posterior to that final arch, we´re going to have the opening of the airway, the laryngotracheal groove and just on the opposite side of that, we´ve got the esophagus. 01:58 So the mouth, throat, and airway, and esophagus are present in this area. 02:04 But for the tongue to form, we´ve got to have a few different things happen. 02:08 First, the lateral and median lingual swellings enlarge tremendously and start sticking out the front part of the early mouth. 02:16 As the mucosa migrates, the third arch grows over the second arch and completely obliterates the copula. 02:24 As that´s occurring, the third and fourth arch move forward and the hypopharyngeal eminence joins the back end of the median lingual prominence. 02:37 So they´re all growing together and the tongue muscles are fusing together at this point. 02:41 Now, one interesting thing that´s occurring here is that the second arch is completely obliterated but the bits of its mucosa migrate on to the first arch and are gonna become the taste buds of the anterior two thirds of the tongue. 02:54 So here, we can see that in blue, the anterior two thirds of the tongue have a core of skeletal muscle, innervated by cranial nerve 12. 03:03 But the mucosa is innervated by cranial nerve five, the mandibular branch of the trigeminal nerve. 03:10 Because it´s a first arch structure, it´s gonna be innervated by that nerve. 03:14 However, scattered along it are little bits of the taste buds innervated by the chorda tympani nerve which is a division of the facial nerve. 03:24 Now, since the second arch was otherwise overgrown, the posterior third of the tongue is made up of third arch derivatives and it´s gonna be innervated by the glossopharyngeal nerve, cranial nerve number nine, but at its core, once again is skeletal muscle derived from the occipital somites and innervated by cranial nerve 12 and the very, very far end near the epiglottis at the base of the tongue, we´ve got the fourth arched derivatives which are gonna be innervated by the vagus nerve. 03:54 Now, what can go wrong in this process? As the tongue grows forward, it typically has a free edge so it can extend out the mouth. 04:02 If the frenulum that anchors the tongue to the base of the mouth is a little too far anteriorly, the tongue is literally tied to the floor of the mouth. 04:11 This is called ankyloglossia or being tongue tied and it can be fixed by actually releasing that excessive frenulum. 04:19 So cutting through it so the tongue can extend out the mouth. 04:21 Less commonly, the two lateral lingual swellings sometimes don´t fuse and you wind up with a bifid or forked tongue. 04:29 This is very uncommon but it does happen. 04:32 Now, the next interesting thing involving the tongue is that when the first arch and second arch meet, there´s a small little divot right at their point of juncture and that is called the foramen cecum. 04:45 And initially, during early development, it actually has a very deep pit and at the base of that pit is something called the thyroid diverticulum. 04:54 This little tube is going to form the thyroid gland and it´s going to move inferiorly from the tongue down the neck, to take up its position in front of the trachea. 05:05 So the thyroglossal duct is the name of that tube that connects the foramen cecum of the tongue to the developing thyroid gland. 05:14 So the thyroid gland gets larger and larger as it moves down from the foramen cecum. 05:19 Now, it´s said that this migrates inferiorly. 05:22 What´s really happening is it´s tied to developing structures here and the body elongates around it, stretching it out, and eventually, separating it from the base of the tongue as it "descends", it´s going to pass the hyoid bone, the laryngeal cartilages, and come to rest just on the anterior trachea. 05:41 Funnily enough, right where my bowtie is hanging out there. 05:44 And just like the bowtie, it´s gonna have a left and right lobe that will take up kind of residence right here on either side connected by an isthmus right in the middle. 05:55 So the thyroglossal duct that connected the thyroid gland to the tongue generally gets obliterated and we don´t have any direct connections between the tongue and the thyroid gland once the development has completed. 06:08 However, you can occasionally have bits of thyroid tissue get left along the path of descent. 06:16 This generally doesn´t create any problems unless the thyroid gland has a pathologic process associated with it like hashimoto's where you have an autoimmune reaction to the thyroid tissue or hyperthyroid conditions where it´s too active. 06:30 Occasionally, the thyroid gland can be completely separate but a strip of it can extend up the midline following the pathway of the thyroglossal duct. 06:40 This is referred to as a pyramidal lobe. 06:43 So instead of a left and right lobe, we´ve got a third one sticking straight up. 06:47 This is only really problematic if you have to do any sort of a laryngeal access or airway access and encounter thyroid tissue along the way. 06:56 You can have cysts of thyroid tissue present anywhere along its point of migration and these thyroglossal duct cysts can sometimes get aggravated and enlarged and people don´t tend to like it when something in their neck gets aggravated and painful and they will tend to go see a doctor for that and you may find thyroid tissue in that area. 07:18 Particularly, in the region just in front of and inferior to the hyoid bone. 07:24 Alright, thank you so much and we´ll catch you on the next talk.
About the Lecture
The lecture Development of Tongue and Thyroid Gland by Peter Ward, PhD is from the course Development of the Nervous System, Head, and Neck. It contains the following chapters:
- Development of the Tongue
- Toungue Abnormalities
- Development of the Thyroid Gland
Included Quiz Questions
The motor innervation of the tongue is supplied by which cranial nerve?
- CN XII
- CN XI
- CN X
- CN IX
- CN VII
The anterior 2/3rds of the tongue are derived from which pharyngeal arch?
- First
- Second
- Third
- Fourth
- Sixth
What congenital condition occurs when the lateral lingual swellings fail to fuse?
- Bifid tongue
- Ankyloglossia
- Aglossia
- Macroglossia
- Hypoglossia
What embryonic structure connects the foramen cecum to the developing thyroid gland?
- Thyroglossal duct
- Thyroid diverticulum
- Laryngotracheal groove
- Hypopharyngeal eminence
- Copula
Author of lecture Development of Tongue and Thyroid Gland

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I never enjoyed a lecture about embriology like this before. love it!
