Playlist
Show Playlist
Hide Playlist
Development of Larynx and Large Airways

-
Slides 06-36 Development of the large airways.pdf
-
Reference List Embryology.pdf
-
Download Lecture Overview
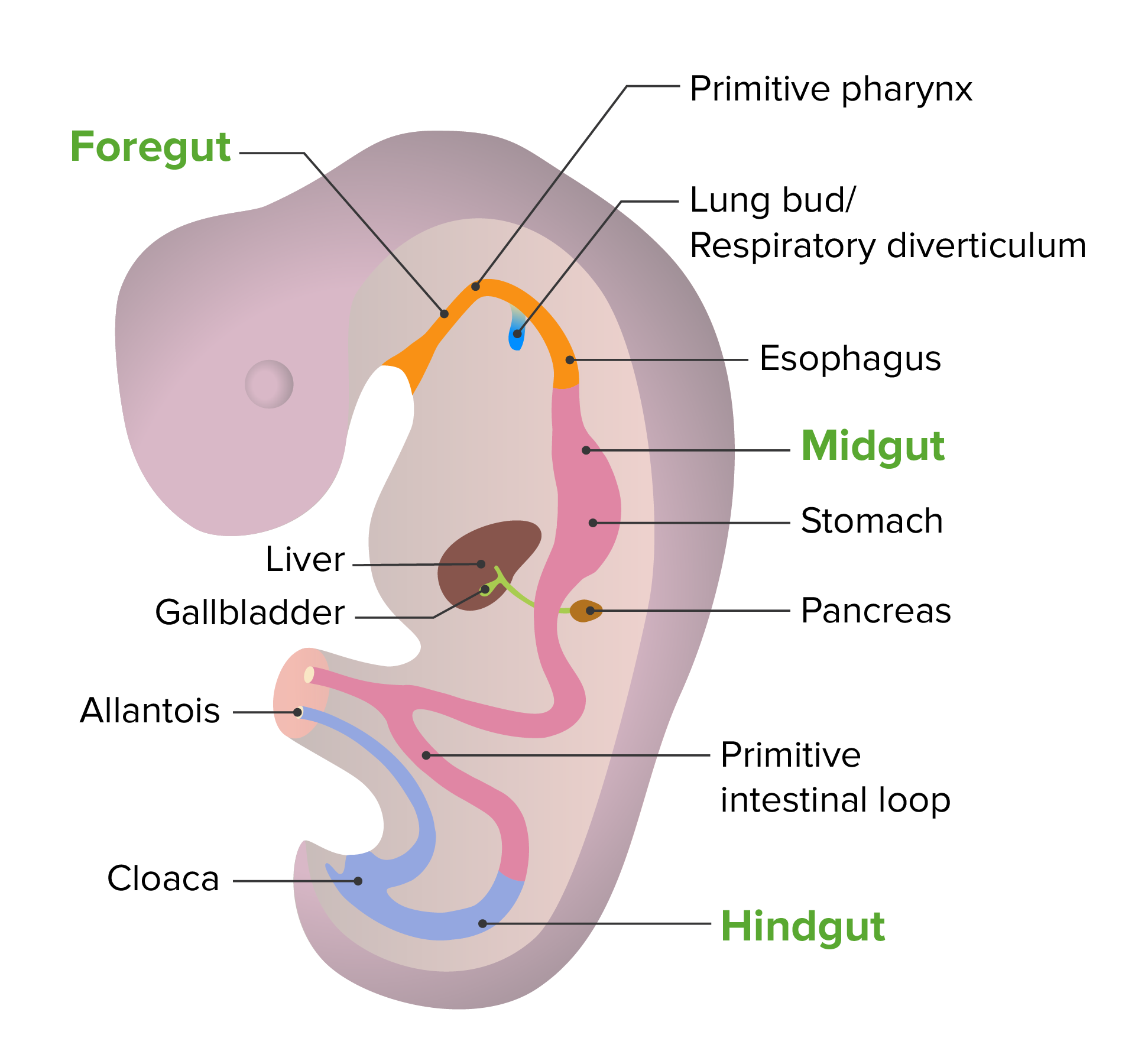
00:01 Now, at the laryngeal inlet, we're going to have the first separation of food and air into separate chambers to travel down to the lungs or the stomach respectively. 00:12 As the tongue and oral cavity develop, the epithelium inside the mouth actually proliferates to a really, really marked extent and it will actually cover the laryngeal inlet. 00:23 Fortunately, as our mouth and our whole body gets bigger, that inlet re-canalizes and reopens. 00:31 And in the process, that little thin membrane that briefly covered the laryngeal inlet reopens and we're now able to start pulling amniotic fluid into our lungs and giving our respiratory system a workout. 00:43 And one little trivia on a side of this is that the remnant of that fold still exists in our larynx. 00:51 That's the false vocal fold. 00:52 That's where that little covering had existed and the little divot of space beneath it is called the laryngeal ventricle. 01:00 Those are both remnants of the point where it was completely covered over and then, reopened. 01:05 Let's return to the respiratory diverticulum and follow it. 01:09 As you may know, we have two lungs. 01:11 We don't just have a single midline structure going down, down, down. 01:15 Eventually, it's gonna split and it splits into two primary bronchi during week five and these continue invading the surrounding mesoderm. 01:23 One thing to notice that the respiratory diverticulum is covered by endoderm and that endoderm is only gonna form the inner lining of the respiratory tract. 01:35 It doesn't actually make the connective tissue structures of the lung. 01:38 That's coming from the surrounding mesoderm. 01:41 So the mesoderm is gonna be made of loose connective tissue, mesenchyme that's undifferentiated but becomes further and further directed to become lung tissue as the branching of the respiratory bud continues. 01:55 So we have a right and left primary bronchus on week five. 01:58 In week six, they're going to split into three secondary bronchi on the right and two secondary bronchi on the left. 02:06 And if you know your anatomy, you know that we have three lobes on the right and two lobes on the left. 02:12 So that makes sense and is mirrored by the embryonic development. 02:16 But we're not done. 02:17 In week seven, each of those secondary bronchi have additional branches called tertiary bronchi and these are gonna supply individual broncho-pulmonary segments that go to specific regions of the lung and carry a pulmonary artery branch with them. 02:34 Now, at that point, we're gonna have continued fine division of the airway into smaller and smaller pieces. 02:42 We're not gonna follow it by name but you should know that there's roughly 23 generations of branching that are going to occur by the time we're born to take that air into smaller, and smaller, and smaller spaces until we eventually have gas exchange able to occur at the alveoli. 02:59 Now, looking at this microscopically, we're gonna see that the endoderm lining the airway is surrounded by splanchnic mesoderm. 03:07 As we mentioned already, that mesoderm is gonna become the connective tissue structures of the lung in the larynx, trachea, and bronchi. 03:15 That includes some cartilaginous rings or plates. 03:19 The cartilage is gonna allow our airway to stay open. 03:22 If we just had a loose tube every time we breathe heavily and had a lot of flow through there, that tube would tend to collapse and we don't want that to happen to our airway. 03:32 So the cartilage holds the large airways open, maintains a little bit of rigidity so that we're able to keep our airway going even when we're running fast and have a lot of air travelling through there. 03:43 In the larynx, we form all the laryngeal cartilages like the thyroid cricoid cartilage, etc. 03:48 In the trachea, we have C-shaped rings of cartilage and then, in the bronchi, not so much rings but cartilaginous plates and by the time we get to bronchioles, the smaller airway, we're gonna have no cartilage in the plate, or no cartilage plates in the airway, but the small diameter is gonna make sure that those don't collapse and the connective tissue of the lungs actually tends to hold those smaller airways open. 04:13 So what can go wrong in this process? The first set of things that can go wrong is that we can have failure of that larynx to recanalize. 04:22 Remember that early on, the oral cavities' epithelium covered the laryngeal inlet but then, ruptured. 04:28 If it does so incompletely, it can create a very small opening and this is called congenital subglottic stenosis. 04:35 And essentially, it's gonna make breathing a little bit more difficult. 04:38 Possibly result in some noise as the infant is trying to breathe quickly and move air in and out of the lungs. 04:44 Another problem that can occur is instead of a small opening, we can have little webs of tissue stretching across the laryngeal inlet. 04:52 These laryngeal webs don't necessarily cause too much trouble but you might note them on examination. 04:58 But if they're covering a significant amount of the airway, they can create some noise as the patient is gonna breathe. 05:03 Generally, these are relatively easy to repair. 05:06 You just have to go in, cut the webs, or open up the subglottic stenotic airway just a bit more to allow gas to flow easily. 05:15 Very commonly, you can have failure of the cartilages in the larynx, the trachea, and the bronchi to be completely solid by the time birth happens. 05:26 This is not uncommon and results in laryngomalacia, tracheomalacia, or bronchomalacia, and the best way to keep those straight is just to remember that malacia means floppy. 05:36 So if you have a floppy larynx, it's going to be a little more able to collapse during heavy breathing. 05:43 So laryngomalacia is the most common anomaly of this airway. 05:46 The upper airway is gonna have that fairly prone and generally, you're going to have the airway close when someone's breathing quickly or laying flat, laying supine. 05:57 So if they're laying on their back and they start breathing in a labored way or having difficulty breathing, it could be a sign of laryngomalacia. 06:05 Tracheomalacia is exactly the same thing but affecting the rings of the trachea and this is gonna be closing whenever quick breathing is occurring and might result in wheezing, coughing, and interruption of the airway. 06:19 And last but not least, if the bronchi have a segment that's got some malacia going on, it will also tend to close and cause some wheezing and other problems related to that like coughing, backup of mucus into the area. 06:32 The good news regarding all of these conditions is that they tend to improve as time goes by. 06:36 The cartilage in the larynx, the trachea, and the bronchi will tend to become more firm with age so long as you follow your patient's progress and make sure that they're supported in the process, it will tend to resolve on its own. 06:49 Thank you very much for your attention and I'll see you on our next talk.
About the Lecture
The lecture Development of Larynx and Large Airways by Peter Ward, PhD is from the course Development of Thoracic Region and Vasculature.
Included Quiz Questions
The respiratory diverticulum extends inferiorly and splits into the left and right primary bronchi during what week of embryonic development?
- 5th week
- 2nd week
- 3rd week
- 4th week
- 6th week
Failure of the laryngeal inlet to fully open will cause what condition?
- Subglottic stenosis
- Choanal atresia
- Tracheoesophageal fistula
- Laryngomalacia
- Esophageal atresia
What is the most common congenital anomaly of the upper airway?
- Laryngomalacia
- Tracheomalacia
- Subglottic stenosis
- Tracheoesophageal fistula
- Choanal atresia
Author of lecture Development of Larynx and Large Airways

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
