Playlist
Show Playlist
Hide Playlist
Derma Case: 52-year-old Woman with Fever, Arthralgias, and Painful Bumps

-
Slides Erythema Nodosum.pdf
-
Reference List Dermatology.pdf
-
Download Lecture Overview
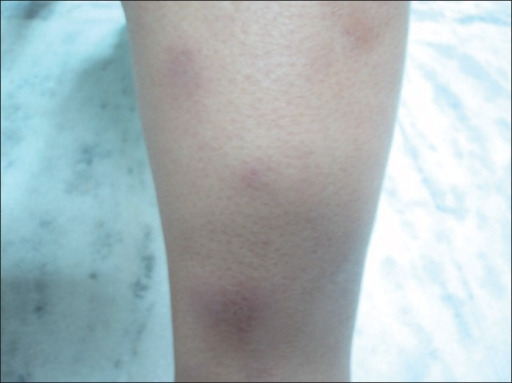
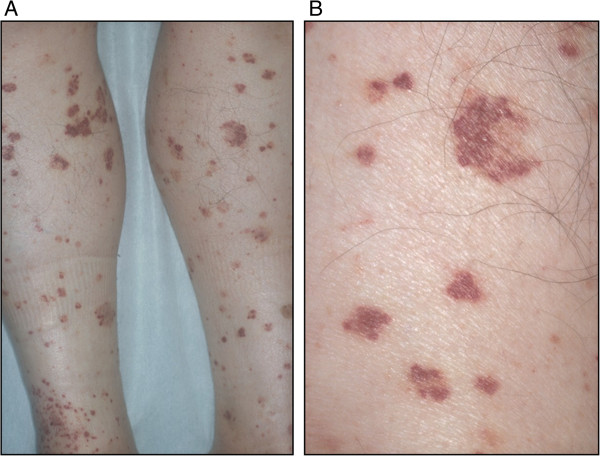
00:02 Next up, we're going to talk about erythema nodosum. 00:06 So, let's jump into our case. A 52-year-old flight attendant with a history of recently-acquired Hepatitis B infection on entecavir presents with fevers, arthralgias, and painful bumps on both of her legs. 00:21 Now, she started the entecavir about 3 weeks ago, and all her symptoms began about a week ago. No joint swelling, and she also admits to intermittent abdominal pain exacerbated by eating. 00:33 No other skin involvement. She's a non- smoker, no alcohol or illicit drugs. 00:38 The family history is non-contributory, and on review of systems, she reports some weight loss, some fatigue, and malaise but no dyspnea or coughing, and no eye symptoms. 00:49 So pulling up our 4 important variables, seems like the time course is sub-acute. 00:53 This has been basically happening for a week, maybe up to 3 weeks. 00:58 Pattern of skin involvement seems to involve the lower extremities predominantly, and it is symmetrically involving the lower extremities. 01:05 And it sounds like there's some evidence of skin inflammation, based on the fact that she's got some painful bumps on both of her legs, as opposed to just hyperpigmentation. 01:15 And importantly, weight loss, fatigue, malaise, something systemic is going on, so that's going to frame our differential as well. 01:24 Physical exam. She is febrile, just about, 100.2°F. 01:30 Little bit tachycardic at 92, blood pressure's 155/104. 01:35 No evidence of any scleral icterus or an involvement of asclera. No lymphadenopathy. Pretty much benign cardiopulmonary exam. 01:42 Her abdomen, despite having some kind of postprandial discomfort, is soft, non-distended, non-tender. 01:49 Musculoskeletal exam is non-focal. Neural exam, same. 01:54 Skin and nail exam we see numerous tender purpuric papules on the calves with associated erythematous nodules. 02:04 No nail findings and no other skin lesions. Creatinine's up a little bit at 1.4. Urinalysis with a little bit of protein. 02:13 ANA, importantly, is negative. LFTs are normal. 02:17 2+ blood, no casts on her urinalysis HIV is negative. Her ESR, a bit elevated at 48. 02:26 And her hemoccult test is positive, certainly making us a little bit more concerned about this prandial abdominal pain that she's been experiencing. 02:35 Chest X-ray, unremarkable, and there's a picture for us. 02:40 So, which of the following is the most likely diagnosis? Well, erythema nodosum. Boy, I'm really tempted to pick the first item on our list because that's the name of our video here. And in addition, it's associated with a number of different conditions, whether it's certain infections or inflammatory bowel disease, other autoimmune things. 03:03 There's a variety of things that we oftentimes will see with erythema nodosum, sarcoidosis, for example. 03:10 Nothing that we're obviously getting from our case, so far. 03:14 We don't typically think of hepatitis B as being a trigger for E. nodosum. 03:18 But we do know it can be precipitated by a number of medications. 03:22 Now, entecavir, not one that I would normally think of for that, but certainly, we'll have to keep this on our list. Moving on to lupus. 03:31 This is certainly a multi-system disease with potentially renal and skin involvement amongst a number of other organs. 03:38 It does have a female predominance as we're seeing in our patient. And it is typically, though, more common in younger patients. 03:46 And in the United States, in particular, among African-American women where it's 9 times more common than in, for example, a Caucasian male. 03:56 Importantly, though, right off the bat, lupus is pretty much thrown off our list by virtue of the negative ANA test. It's not unheard of to have a negative ANA, but pretty darn close. 04:09 So let's X that one out. Next up, mycosis fungoides, also known as cutaneous T-cell lymphoma. Now, it can present in nearly any way that it wants to. It does have a predilection for the lower extremities as we're seeing in our patient. 04:24 That being said, while lymphoma can occur at any age, it's pretty unusual to occur in a patient of our -- to occur in the age of our patient. 04:34 The onset was also too rapid. We expect a much more indolent course over the span of many months for cutaneous T-cell lymphoma or mycosis fungoides. And the fact that on physical exam, the patient had no evidence of lymphadenopathy, would also steer us clear of that diagnosis. 04:52 Let's talk about polyarteritis nodosum. Polyarteritis nodosum. 04:56 Now that is a medium-vessel vasculitis, and I think it's definitely worth our consideration. We're going to have to talk about that one a bit more on the next slide. But first, quick look at thrombophlebitis. It can certainly cause painful calves, as we're seeing in our patient, though bit unusual to have it occurring bilaterally at the same time. 05:16 And calves, or thrombophlebitis, doesn't typically explain the fevers that she's having, the arthralgias, certainly not the heme-positive stool. So, all in all, thrombophlebitis seems pretty unlikely to explain our patient's symptomatology.
About the Lecture
The lecture Derma Case: 52-year-old Woman with Fever, Arthralgias, and Painful Bumps by Stephen Holt, MD, MS is from the course Allergic and Immune-mediated Skin Disorders.
Included Quiz Questions
Which of the following is associated with erythema nodosum?
- Symmetric distribution
- Mucosal involvement
- HBV infection
- Nodules developing over several weeks
- Medium vessel vasculitis
Thrombophlebitis commonly presents with which of the following?
- Calf tenderness
- Bilateral pretibial nodules
- Gastrointestinal abnormalities
- Renal dysfunction
- Lymphadenopathy and constitutional symptoms
Which of the following is associated with mycosis fungoides?
- Lymphadenopathy
- Fungal infection
- Acute onset
- A predilection for the upper extremities
Author of lecture Derma Case: 52-year-old Woman with Fever, Arthralgias, and Painful Bumps

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
