Playlist
Show Playlist
Hide Playlist
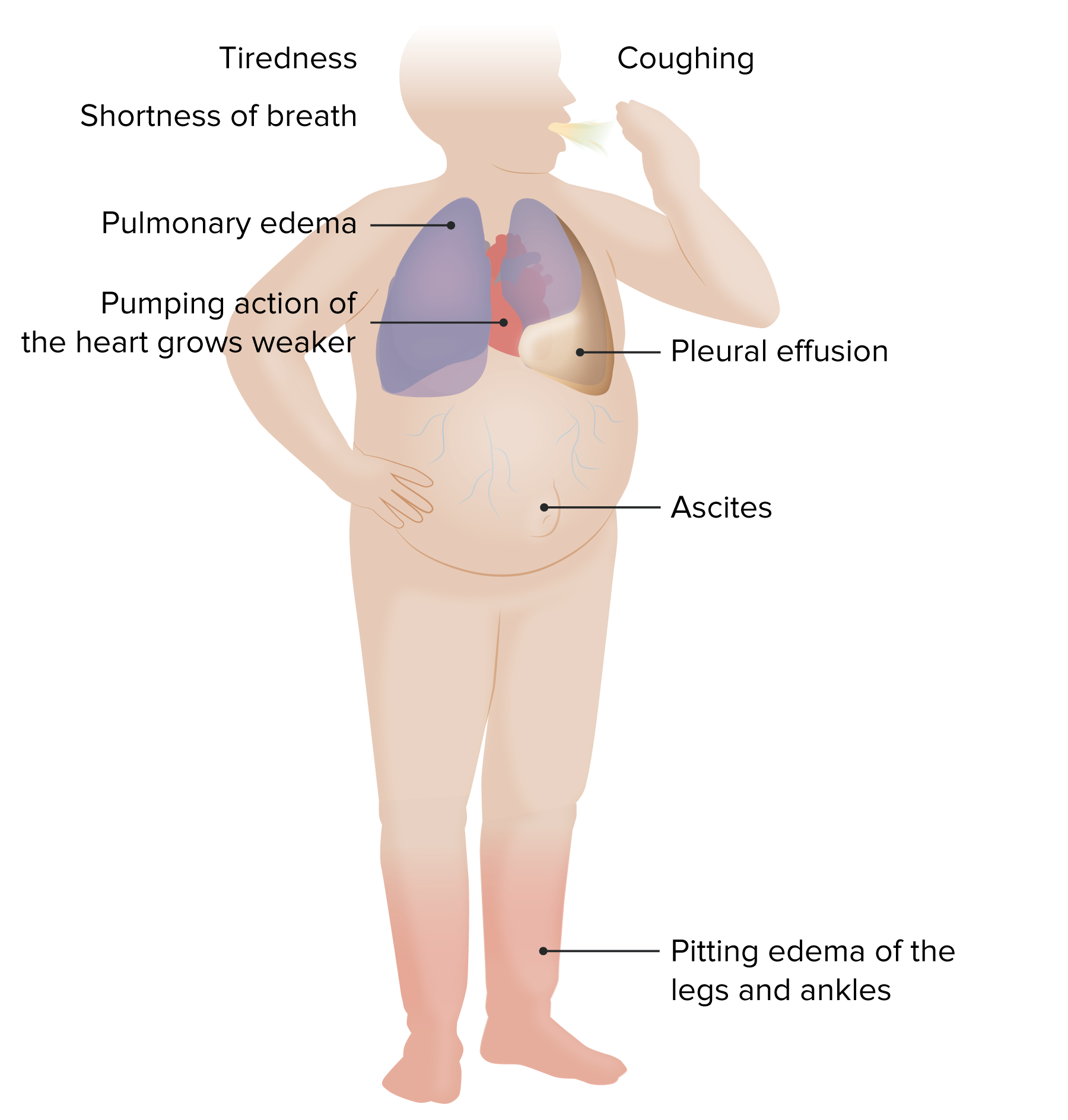
Heart Failure (HF): Signs and Symptoms

-
Slides CongestiveHeartFailure CardiovascularPathology.pdf
-
Download Lecture Overview
00:00 Now, signs and symptoms of dysfunction. If your left ventricle is not working properly, then what kind of issues as your patient coming in with please? Pulmonary. What does that mean? Pulmonary edema, orthopnea. What does that mean? "Hey doc, when I go to bed, I have this beautiful beautiful bed that I bought, nice foam bed and you know which is fantastic, but I never get a chance to use it. And whenever that I do it at night, I feel like I cannot breathe. So after placed four pillows underneath my bed, now at this point, I have to sleep on my recliner. Can’t even use my bed. You know how bad I feel." Welcome to orthopnea. Or "Hey doc, I sleep at night and I can’t breathe. I have to run out to the window, open it and I have to take a breath of air." This is PND, paroxysmal nocturnal dyspnea. This then to you signifies failure of what side of the heart? Left side of the heart, backup into lungs. Welcome to transudate pulmonary edema. Worst case scenario. You have blood that is now escaping into the lung in parenchyma. These are called heart failure cells or hemosiderin-laden macrophages. All the macrophages do is they come in and they are going to gobble anything that is in that particular environment, maybe it is coal. Later on we will talk about coal workers pneumoconiosis, those macrophages will gobble up coal. And here it is blood in hemosiderin. So different places in which macrophages, atherosclerosis. 01:32 Forgot about that one, almost. Macrophages come in and they gobble up LDL or cholesterol. 01:39 Welcome to foam cells. So in general, just understand the concept. What if it is right ventricular dysfunction? Now I get into circulatory issues on the systemic side. So we have positive JVD. You might have pitting edema before we get into anything further and it is important that you pay attention to the official New York Heart Association Classification. 02:01 Now class I. Symptoms only with maximal exertion. So we're the process of congestive heart failure, but we were going through different classes and in your mind, you might want to bring that graph that we just reviewed in great detail to then help you explain the different classes. 02:20 So imagine now you are moving clockwise. Why did the performance decrease? Because of decreased contractility. At some point, the contractility may then be improved. That is so much of contractility, but the performance might be improved because of an increase in volume due to compensation. 02:37 We will talk about aldosterone. Symptoms with moderate exertion class II, moderate. Minimal. 02:44 Now we're getting worse. Even minimal exertion is then going to exacerbate the issues of heart failure. And then symptoms at rest. Where are you? Pay attention to class III and class IV. Ladies and gentleman, the parallel that I wish to bring here as well is that there will be particular WHO classifications that is imperative for you to keep in mind when dealing with what is known as pulmonary arterial hypertension. And the reason I say that is because when it comes to pharmacology management, they will then ask you and all they put in there is "Your patient has congestive heart failure showing symptoms of class III and class IV." Or "Hey, I have a patient and the patient is now exhibiting symptoms of class II, class III of pulmonary arterial hypertension." So it is important that you pay attention to some of these guidelines. They are created on purpose and you must understand the clinical significance of it. You begin here with NYHA. 03:48 Physical examination. Left sided everything is pulmonary. Crackles.
About the Lecture
The lecture Heart Failure (HF): Signs and Symptoms by Carlo Raj, MD is from the course Heart Failure: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following symptoms is associated with right-sided heart failure?
- Peripheral edema
- Orthopnea
- Pulmonary rales
- Paroxysmal nocturnal dyspnea
- Foam cells
What are heart failure cells?
- Hemosiderin-laden macrophages
- LDL-laden macrophages
- Cholesterol-laden macrophages
- Coal-laden macrophages
- None of the other responses are correct.
According to the New York Heart Association classification, which class of heart failure would describe a patient who experiences symptoms after walking 10 meters?
- Class III
- Class I
- Class II
- Class IV
- Not enough information to say
Author of lecture Heart Failure (HF): Signs and Symptoms

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
