Playlist
Show Playlist
Hide Playlist
Hypertrophic Cardiomyopathy: Complications, Morphology, and Histology

-
Slides Cardiomyopathy.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
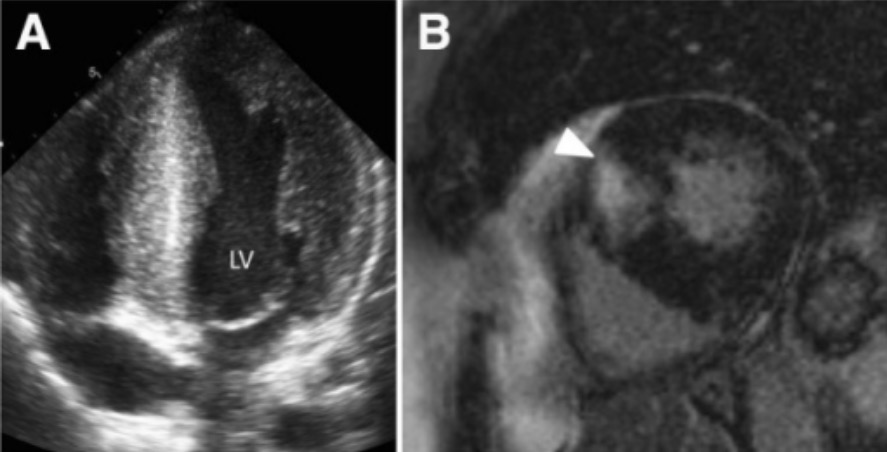
00:01 What do we see on EKG? Well, first of all, we see increased muscle mass. 00:06 So there'll be a very prominent QRS complex, so very high peaked waves. 00:12 You will also or you may see atrial fibrillation due to the dilation of the left atrium, and leading also potentially to mural thrombus formation. 00:24 Ultimately, ventricular fibrillation that can cause sudden cardiac death can be one of the in fact primary manifestations of hypertrophic cardiomyopathy. 00:35 Because the mitral valve is thickened and it's abnormal, there's going to be an increased propensity to developing infectious endocarditis of the mitral valve. 00:43 And of course, because the left ventricle is not getting adequate forward flow, and there is regurgitant flow, patients will present potentially with congestive heart failure, shortness of breath, etc. 00:59 What does this look like, grossly? So in this particular case, we're showing you the left ventricle. 01:05 This is the anterior half of the heart. 01:07 And there is relatively greater thickening of the septal muscle compared to the lateral left ventricular wall, which is all the way over on the left hand side. 01:17 There will be focal scarring, again, because we're not getting good perfusion. 01:22 Out the coronary arteries, we can get areas of larger fibrosis, but also we're going to have increased interstitial fibrosis, because of the pressure volume overload or the pressure overload on the cardiac fibroblasts. 01:38 This image is showing that plaque of systolic interior motion. 01:41 We have lifted up the anterior leaflet of the mitral valve and reflected that so you can see underneath where we're pointing, that's the left ventricular outflow tract right behind that leaflet is the aortic valve. 01:55 And now we are seeing the evidence of that plaque, or the anterior leaflet flapping recurrently up against the septum. 02:04 And you can imagine that when that happens, we closed left ventricular outflow tract prematurely. 02:10 And we end up with diminished cardiac output. 02:14 Histologically this is the myocyte disarray. 02:17 This is a very low power shot but you get a sense that this is not uniform kind of lining up in the myocytes, that they kind of look like a herringbone pattern, with kind of branches going in various ways. 02:30 Individually, the cardiac myocytes are also huge. 02:33 So the the nuclei of the cardiac myocytes are 10, 5 to 10 fold greater than the normal size, saying that these cells individually are huge. 02:44 You also see some lighter pink, in between the cardiac myocytes and that actually represents the interstitial fibrosis. 02:51 We can accentuate that interstitial fibrosis by doing special trichrome stains. 02:56 Trichrome is a histologic staining procedure that highlights collagen as blue. 03:04 So you can see that all the spaces in between, in fact are increased interstitial matrix deposition. 03:10 And as mentioned previously, we can also get hypertrophy of the intramyocardial arterioles and so that wall is markedly thickened, that's what's in the green circle. 03:22 Those are the histologic changes. 03:24 The buzzword you want to remember for the boards is myocyte disarray with increased interstitial fibrosis.
About the Lecture
The lecture Hypertrophic Cardiomyopathy: Complications, Morphology, and Histology by Richard Mitchell, MD, PhD is from the course Cardiomyopathy.
Included Quiz Questions
What histologic finding is seen with hypertrophic cardiomyopathy?
- Interstitial fibrosis
- Myocyte hyperplasia
- Thin myocardial arterioles
- GIant cells
- Aplasia
Author of lecture Hypertrophic Cardiomyopathy: Complications, Morphology, and Histology

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
