Playlist
Show Playlist
Hide Playlist
Coma and Brainstem Reflexes


-
Slides 10 AlteredMentalStatusandComa Neuropathology II.pdf
-
Download Lecture Overview
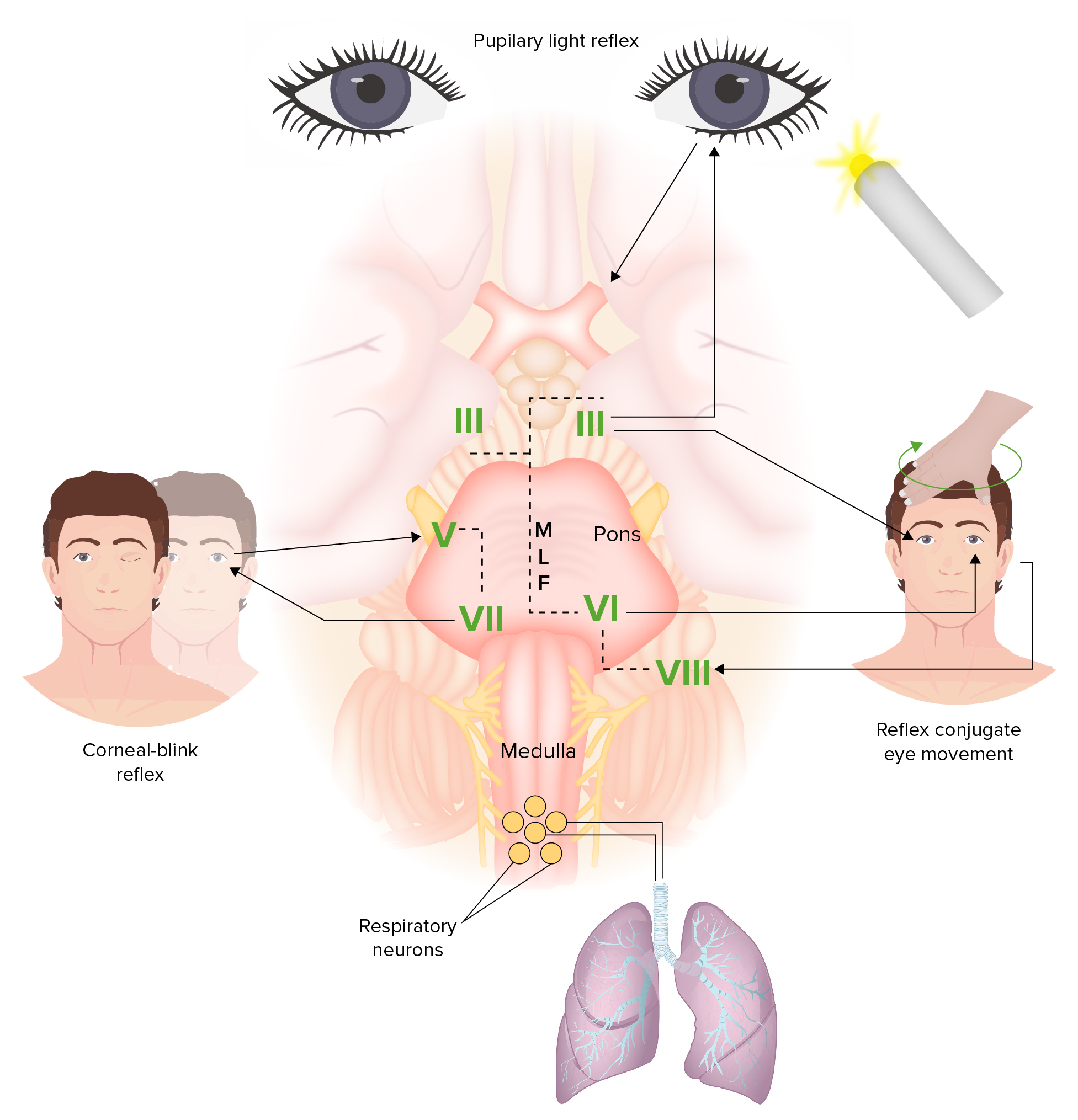
00:01 What’s a coma, the definition? A state of unarousable unresponsiveness. 00:09 Describes the level of consciousness in terms of response to the various levels of stimuli. 00:14 And patients with only reflexive responses may still be described as being in a coma. 00:19 So, reflexes could be intact but still will be in a coma. 00:23 May be due to diffuse cerebral insult or to the focal processes. 00:30 Examining the possibility of comatose patient. 00:34 We have to say/yell patient’s name, verbal stimulation. 00:39 Shake/tap, this is tactile stimulation. 00:43 Press on patient’s nail beds, and this is peripheral painful sensations or stimulation. 00:49 Sternal rub or nasal swab, we call this central painful stimulation. 00:55 And if these tests fail to reveal a response, your patient is possibly in a coma. 01:02 The brainstem exam is done to determine if the brain death is present. 01:06 Remember, you ask yourself how awake is your patient if you’re thinking about level of consciousness. 01:12 At this point, obviously, functionality has been lost, not cognition. 01:17 Cognition has been lost. 01:20 So, what are some of these brainstem reflexes that we’re paying attention to? Remember please, the pupillary light reflex. 01:26 The afferent, referring to optic nerve, is going to then take in the stimuli of light. 01:33 And the efferent is going to come way of oculomotor, parasympathetic, therefore, causing constriction of your pupil. 01:40 Your brainstem functioning, pupillary light reflex. 01:44 We have known as oculocephalic reflex or doll’s eye. 01:49 And with this, the afferent here is going to be your eighth cranial nerve, which is your vestibulocochlear. 01:55 The efferent would be through your oculomotor, and then you have your trochlear and abducens all in the form of your eye, in which if you have oculocephalic or doll’s eye, then everything should remain within stable or balanced. 02:11 You have a corneal reflex, here literally, you’re going to touch. 02:15 So, the afferent would be through your trigeminal, ophthalmic branch, and then with the closure of your eyelid, that would be from your facial. 02:23 Your corneal reflex, you touch your cornea, and then there should be blinking. 02:29 The gag reflex, afferent would be through your glossopharyngeal. 02:34 Take a swab or whatnot, touch the back of the throat. 02:37 And then the efferent would be through your vagus. 02:40 These are all important brainstem reflexes. 02:42 Remember please, at this point, you’re going to try to figure out as to whether or not brainstem functioning is even intact or not. 02:48 Coma. 02:51 And the brainstem reflexes are the cold calorics. 02:55 What happens here? Fifty milliliter ice water injected into the ear, for example. 03:00 Cold is an inhibitory stimulus to the vestibular nerve. 03:05 The vestibular nerve projects to the contralateral, contralateral, sixth cranial nerve or abducens. 03:11 Normal response is slow deviation of eye, eye, towards the side of the cold water, then a fast return to the midline, and that portion is your nystagmus. 03:25 So, towards the cold and then a fast return to the midline. 03:30 In coma, remember here, we’re talking about the cold caloric or we talk about the doll’s eye reflex. 03:37 We have the eighth cranial nerve, and along with this, the pathways are intact. 03:43 The eyes tonically deviate toward the cold stimulus with no fast phase. 03:51 In coma, there is no fast phase to come back to the midline. 03:57 Remember, primitive brain looks to stimulus, higher brain brings eye to the midline, and that is what is lost, please, in coma.
About the Lecture
The lecture Coma and Brainstem Reflexes by Carlo Raj, MD is from the course Altered Mental Status and Coma. It contains the following chapters:
- Coma
- Brainstem Reflexes
Included Quiz Questions
Which two cranial nerves are involved in the corneal reflex?
- Trigeminal and facial nerves
- Trigeminal and glossopharyngeal nerves
- Vestibulocochlear and optic nerves
- Vagus and glossopharyngeal nerves
- Trigeminal and vagus nerve
Which two cranial nerves are involved in the gag reflex?
- IX and X
- X and VII
- V and VII
- VII and V
- IV and VI
Author of lecture Coma and Brainstem Reflexes

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
