Playlist
Show Playlist
Hide Playlist
Clinical Manifestations and TB Case Histories

-
Slides 02 InfluenzaATuberculosis RespiratoryAdvanced.pdf
-
Download Lecture Overview
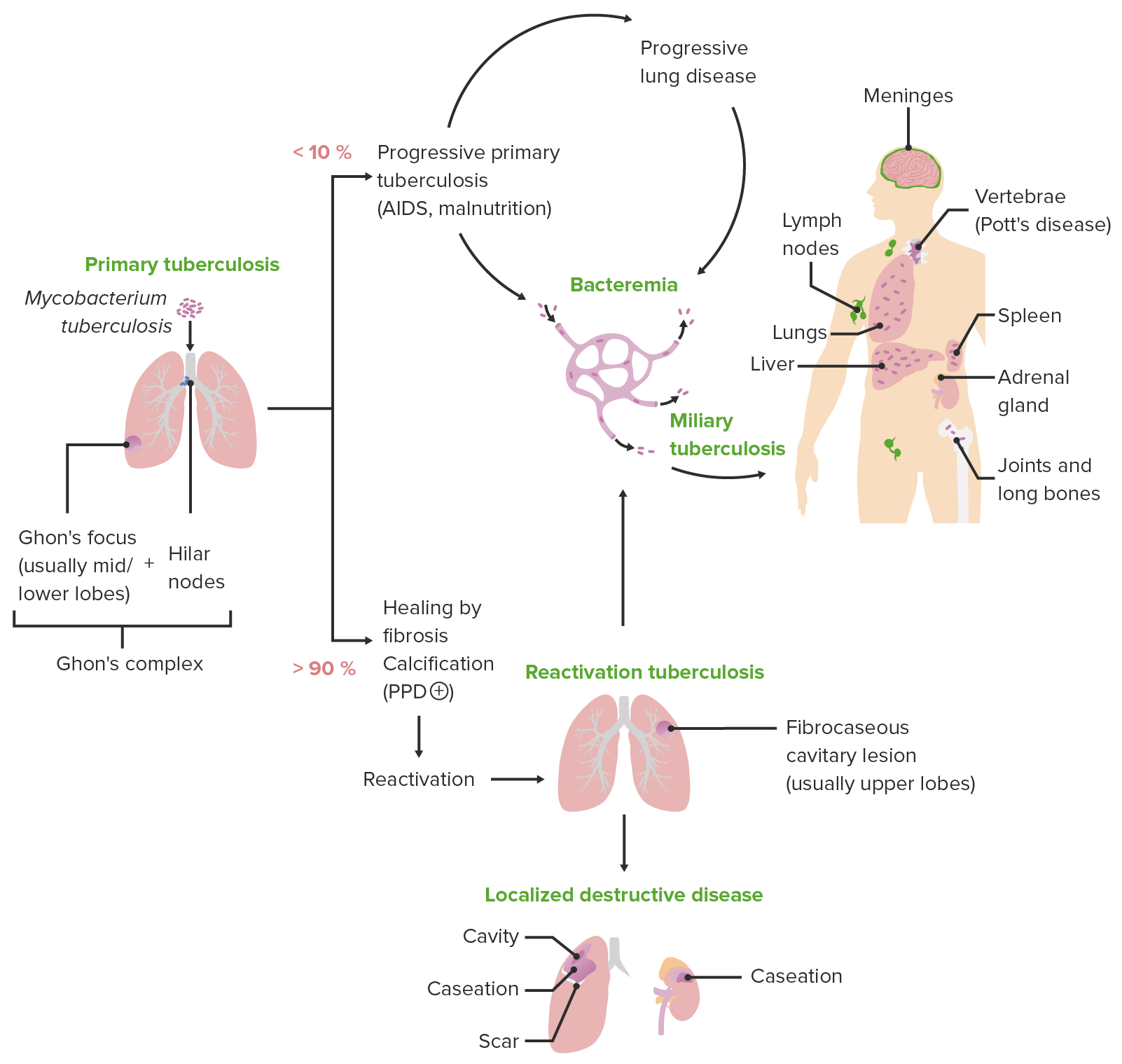
00:00 So the clinical manifestations of tuberculosis are lung alone, pulmonary, which is nearly half the people. A combination of lung plus outside of the lung disease, which is only about 10% of people, and then there's just extra pulmonary disease, disease that is not affecting the lungs, includes the mediastinal lymph nodes, because they are not actually part of the lung, they are in the mediastinum. It also includes pleural tuberculosis, because pleura, the infection is actually of the pleura itself, again that’s not the lung parenchyma. 00:32 Now an important distinction here is that the infective disease of those patients with pulmonary disease and all the extra pulmonary forms of tuberculosis are essentially not infective. You can see there is quite a big list of different sites that can be affected by extra pulmonary disease and the frequency is given here as well. 00:50 The commonest being nodes, lymph nodes, mediastinal lymph nodes, being the commonest sites. 00:56 But It could be pleural, you can have bone and spine disease, you can have miliary tuberculosis which is a very specific form where the tibia has been spread by the blood throughout the body, affecting mainly the lungs, the liver and the bone marrow. Meningitis, which a very serious form but relatively rare fortunately, and then the various parts of the abdomen can be affected as well. So the classic symptoms of someone presenting with pulmonary tuberculosis is very simple, they cough and they may cough with blood present in the sputum, haemoptysis, and with that they’ll have systemic symptoms because it is an active infection and these systemic symptoms are prolonged because the patient presents with several weeks even months’ worth of history. So over that time the patient is feeling ill, they are not eating, and they have fevers and night sweats, and they’ll be losing weight as well. And that's very important for identifying somebody who may have active tuberculosis, the presence of the systemic symptoms. Now the other areas within the thoracic cavity that may be affected are the mediastinal nodes as we've mentioned, but really that doesn't normally cause symptoms of the nodes themselves and is visible on the chest X ray and that sort of patient will present a systemic symptoms but no, necessarily respiratory symptoms. And pleural disease that causes an exudative pleural effusion, and that presents largely with breathlessness and the systemic symptoms that we've described already. 02:20 Now if you have extra pulmonary disease, how you present depends on the site of disease, clearly. So cervical lymph node involvement is very common and those patients will present with a lump palpable in the neck, that they can feel or see themselves. That lump tends to be smooth, its firm and its not particularly hard. If they have mediastinal abdomen lymphadenopathy then that will be identified by X rays. Gastrointestinal disease will cause pain, bloating and ascites. 02:50 Pericardial disease causes a constrictive pericarditis, pericardial effusions.Meningitis presents with chronic headaches, focal neurology and eventually coma, it is a very serious problem with a high mortality and even if you do survive it, you are likely to have a neurological defects as well. Miliary TB I've mentioned is where you have bloodbornes spread across the body and actually that’s very difficult to diagnose because the patient have very few in the way the localizing the symptoms, they just have the systemic symptoms in weight loss, but the chest X ray is often characteristic showing very small nodules throughout both lungs. If you have bone or joint TB that will be presented with a mass and pain of that bone or joint that’s being affected. And if you have nodal TB and bone and joint TB then what can happen is that the infection can penetrate through the skin and cause what we call the discharging sinus, where you have a hole going into the infected area that oozes out fluid, and tuberculosis always can be seen in that fluid. So just to give you a couple of case histories, to give a feel for what this disease and how this disease presents. 03:58 This first patient is a man from India, he has had three months history of systemic symptoms of weight loss, night sweats, and feeling not very well. And with that he's had a cough and if you can see the chest X ray what you can see is bilateral apical disease here, and there is cavitation present and this is a very classical presentation for someone with pulmonary tuberculosis. Systemic symptoms, cough and a chest X ray showing upper lobes changes with cavitation, and given the man was born in India, this is almost certainly going to be tuberculosis because he is from a higher risk group with a real classical presentation of pulmonary tuberculosis looks like and his sputum should show acid fast bacili because this is a high bacillary load, high bacterial load disease. This is a different presentation. This is a Somalian, has moved to London and now he is presenting with two months history of back pain and again systemic symptoms of sweat, feeling not very well and a bit of weight loss. Now the back pain is the localizing symptom for where the problem is and you see this on this MRI scan, there's an area of high density, and in fact if you look closely there is destruction of the edges of those vertebra and there is some soft tissue swelling around those bones and you can also see that there is an angulation occurring there. And this is spinal TB, and the MRI appearance there are very classical for tuberculosis. So again we have somebody from a high risk area, sub-Saharan Africa, so therefore has been exposed to tuberculosis as a child quite likely to have been. Recent emigration, which is a risk factor, systemic symptoms which are very indicative of active inflammatory or infective disease, tuberculosis being one of the common causes and a characteristic radiology. So, just to re-iterate that, to recognize tuberculosis, really you need two things, systemic symptoms plus a high risk group. So somebody's got weight loss, fatigue, fever, sweats who has been born in a high risk country, sub-Saharan Africa, Asia, or is homeless, intravenous drug abuser, alcoholic, has been in a prison, or is HIV positive. With that combination you must think about tuberculosis. 06:14 And the localizing symptoms will help as well, because if somebody has classic localizing symptoms, that will also make the disease much more likely. 06:25 A family history of exposure to tuberculosis is sort of helpful. If somebody says “yes my aunt had TB when I was a child” then that means they are quite likely to have latent tuberculosis but we don’t often get that history.
About the Lecture
The lecture Clinical Manifestations and TB Case Histories by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Infections of the Respiratory Tract.
Included Quiz Questions
Which of the following types of tuberculosis is most likely to be infectious?
- Pulmonary tuberculosis
- Miliary tuberculosis
- Tuberculosis meningitis
- Genitourinary tuberculosis
Which of the following is the most common extrapulmonary site for tuberculosis?
- Lymph nodes
- Pleura
- Meninges
- Spine
- Genitourinary system
Miliary tuberculosis is caused by spread through which of the following routes?
- Blood
- Lymph
- Local
- Skin
- Subcutaneous tissue
Which of the following types of extrapulmonary tuberculosis most commonly presents with constitutional symptoms and few, if any, localized findings?
- Miliary tuberculosis
- Pericardial tuberculosis
- Bone involvement
- Pulmonary tuberculosis
- Pleural tuberculosis
Which of the following is a characteristic appearance of the chest X-ray in pulmonary miliary tuberculosis?
- Multiple very-small nodules throughout both lungs
- Multiple cavitations of the lung unilaterally
- A single nodule in lung apex
- Diffuse fibrosis in lower lung fields
- Multiple large nodules > 1 cm in diameter
Which of the following is probably the LEAST common extrapulmonary site for tuberculosis?
- Myocardium
- Genitourinary system
- Pericardium
- Lymph node
- Gastrointestinal system
A 35-year-old patient who takes refuge in a homeless shelter is diagnosed with tuberculosis. Which of the following is NOT a common symptom?
- Uveitis
- Purulent cough
- Night sweats
- Hemoptysis
- Significant weight loss
A biopsy from the cervical lymph nodes of a patient with constitutional symptoms reveals caseating granulomas. What is the most likely diagnosis?
- Tuberculosis
- Sarcoidosis
- Lung cancer
- Interstitial lung disease
- Pneumoconiosis
Which of the following is the least characteristic radiological sign of spinal tuberculosis?
- Spinal disc herniation
- High-density area
- Destruction of the vertebral edges
- Soft tissue swelling around the affected area
- Angulation
Which of the following is NOT an MRI feature of spinal tuberculosis?
- Circumscribed osteolytic lesions
- Osteitis
- Discitis
- Abscess formation
- Swelling of surrounding soft tissue
Author of lecture Clinical Manifestations and TB Case Histories

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
