Playlist
Show Playlist
Hide Playlist
Classifications of Scoliosis

-
Slides Scoliosis.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
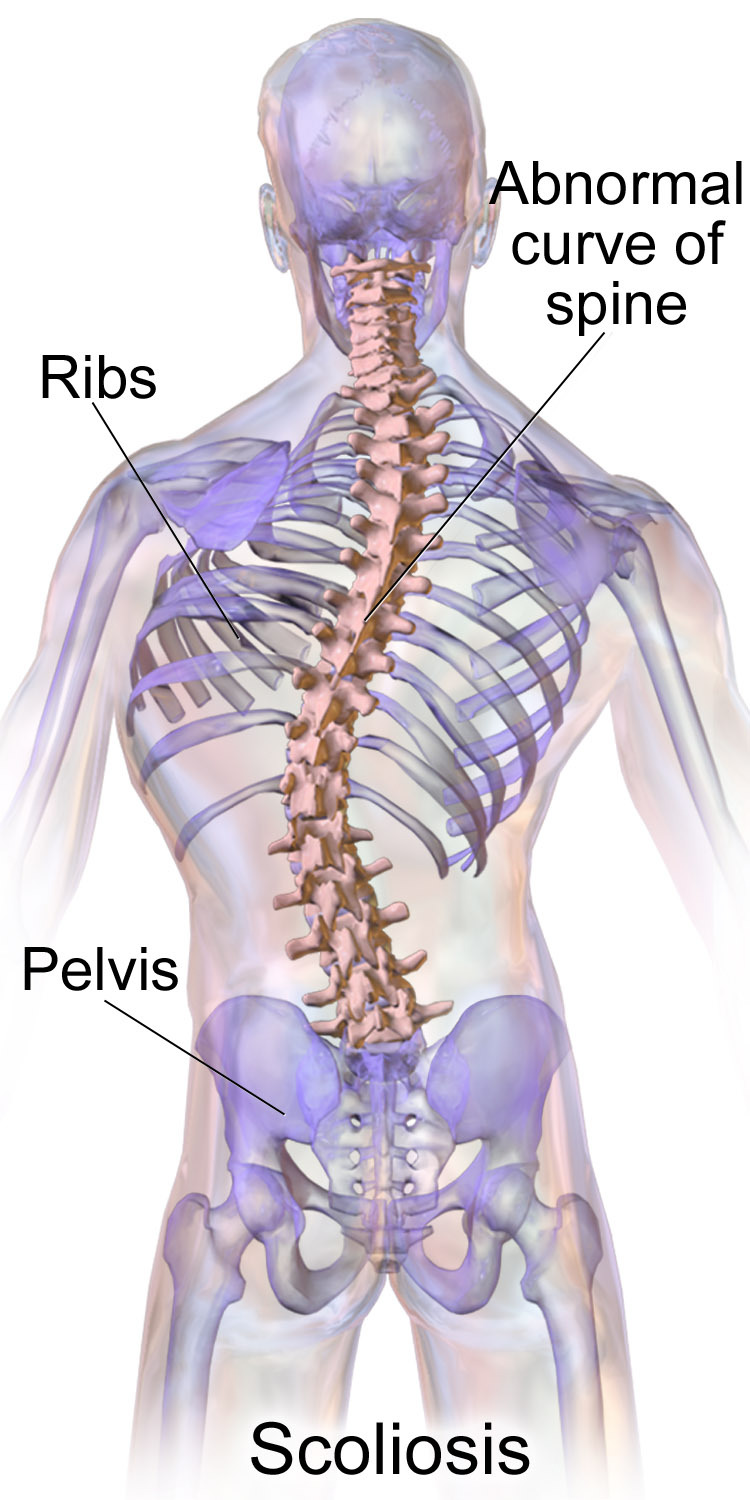
00:00 When we classify scoliosis, we classify it based on a couple of different criteria. 00:07 What is the reversibility? Does it go away with motion and activity? What is the severity? Is it 10 to 20 degrees, 20 to 30? Is it greater than 30 or greater than 50 because it's a different natural history for each of those? Is there an identifiable cause? Is there a muscle weakness or muscular dystrophy? Is osteogenesis imperfecta? Does a student have blue sclera, weakness, Is osteogenesis imperfecta? Does a student have blue sclera, weakness, café au lait spots that might be indicative of a neurofibromatosis? All of those things are clues that the person has a scoliosis. 00:40 We also look at the area of the curvature, as all being very important. 00:47 So if a curve is structural, it does not go away with movement. 00:52 If it is functional, then the curve will go away with particular motions. 00:57 That is when you have a student or a person forward bend. 01:01 If you see it going away, you can call it functional. 01:04 Do you have scoliosis changing from functional to structural? Yes, you can, particularly with an unequal limb length. 01:14 If you have changes in body structure, seeing if there is an amputation or loss of a limb. 01:20 If there is trauma or disk deterioration or degeneration, you can see the change of a functional to a structural scoliosis. 01:29 Fibrosis of the ligaments and fascia can lead to a change and if the person doesn't have full activity or has limited action. 01:37 Those are things that can lead to a change from a reversible scoliosis to a permanent scoliosis. 01:44 When we classify it in the school-based screening, they either have no scoliosis, they have a mild scoliosis of 10 to 15 degrees which we questioned, follow, and want to monitor. 01:56 They may have a moderate scoliosis which is a real noted 10 to 45 degree curvature, at which case the student is going to need a Cobb radiograph or a posterior-anterior radiograph. 02:10 You take an X-ray from behind towards the front and we'll go over how you measure it after that. 02:15 Or is the scoliosis greater than 50 degrees, a real, apparent curvature of the spine that's going to have real and serious lasting effects. 02:24 If you have a curvature greater than 50 degrees, we start looking at how it's affecting the heart and how it's affecting the lungs. 02:31 Those are important complications of a severe scoliosis. 02:36 Most times when a person has a scoliosis, we don't know the cause. 02:40 We don't find the cause. 02:41 It's something that's just uncovered on a screening exam. 02:46 70 to 90 percent of scoliotic curves are idiopathic. 02:50 We don't know the cause. 02:52 As we learn more about scoliosis, we start looking at relatives with scoliosis and other complications including sacral base unleveling or other changes that affect biomechanics. 03:05 So idiopathic is also called infantile, juvenile or adolescent, AIS, adolescent idiopathic scoliosis. 03:14 You can have a congenital scoliosis, an acquired scoliosis, or a neuromuscular scoliosis as well. 03:22 Those are the four different classifications of a scoliosis. 03:25 We do have some general other patterns that we see that are somewhat nebulous and where we classify them. 03:33 In infantile idiopathic scoliosis, it's usually due to gravitational causes, mechanical causes, and the immaturity of the spine. 03:44 We have some bending that is institutionalized or caught in the skeletal system but can go away. 03:52 The ideal treatment with an infantile idiopathic scoliosis is trying to prevent it. 03:57 One of the problems is we see more scoliosis in children when they're put to bed on their back which is the new recommendation for the American Academy of Pediatrics. 04:08 The idea is to prevent sudden infant death syndrome or sleeping sickness of kids. 04:15 Putting them on their back is safer. 04:19 But the parallel to that is there is a slight increase in the amount of scoliosis when children are put to sleep on their back. 04:28 We do treat the curvatures and try and get rid of them as quickly as possible usually with an orthotic and sometimes with the brace. 04:35 The earlier this is done, the better outcome we feel there will be. 04:39 The evidence on this is still being developed. 04:41 We don't have clear, good, definitive answers yet. 04:44 An important reason to diagnose scoliosis early is that when the scoliosis starts can determine what kind of side effects or complications you have. 04:54 If a scoliosis develops before five years of age, it's important to monitor for cardiac or respiratory issues. 05:01 We do know that bony growth is affected by a scoliosis and that you can have a change in the diameter and the size and the shape of the thoracic cavity. 05:10 So the growth of the lungs will be affected. 05:13 Normally there's a tenfold increase in the alveoli from infancy to four years of age. 05:18 This growth in alveoli and lung tissue continues up to eight years of age. 05:23 So scoliosis this early in life can have a definite effect on the lung tissue and lung functioning. 05:32 Juvenile idiopathic scoliosis is when we diagnose it between 4 and 10 years of age. 05:38 This is also a progressive scoliosis much like the infantile idiopathic scoliosis. 05:44 If it's less than 20 degrees, we tend to observe it with an X-ray, a PA, then every 4 to 6 months to see how quick and how severe the progression is. 05:56 It varies widely. 05:58 Some children will not have much progression. 06:01 Once they have that curvature or the blocking of the vertebrae, it tends to stick. 06:07 Others have a gentle twisting and turning that continues over the next few years. 06:13 So it's important to be able to predict what happens. 06:15 That's something you do by monitoring the curvature of the spine on a regular basis. 06:21 If there continues to be progression, then you will consider bracing and stabilization of the spine by external means of which bracing is the most common and most frequently used. While the bracing generally has success when it's done all day long and people don’t get out of the brace, it is the most widely-used non-operative treatment. 06:47 We try not to do surgery at a young age because it does expose the child to other issues. 06:53 It's also not a terminal treatment. 06:55 It's not the end treatment. 06:57 They would require further surgeries later on in life. 07:00 In order to limit the number of surgeries, we do try and delay it. 07:04 One of the reasons we need to monitor juvenile idiopathic scoliosis is checking the top vertebrae for crankshaft phenomenon, looking at the anterior and posterior aspects of the vertebrae and seeing if fusion occurs. We want to avoid fusion of the vertebrae to allow motion. 07:22 The other thing to be aware of is when people do get surgery, generally rodding is done to increase the straightness and prevent further deterioration. 07:34 That's called Harrington rods and that's an attempt to straighten out the spine. 07:41 Adolescent idiopathic scoliosis is thought to be hereditary in that it's seen in families and multiple members of the family. 07:49 It has an association with a hypokyphosis, less of a forward bending hump. 07:56 There are also possible CNS defects that can be seen with this as well. 08:01 There may be a genetic contribution as it is seen throughout families, skipping generations and sometimes skipping parts of the family altogether. 08:09 So it is something that is being watched and studied. 08:12 Patients with AIS will often have a sibling or a parent with scoliosis though. 08:17 We do not have the inheritance pattern of the genetic loci worked out. 08:20 But it has been mapped to chromosome 17 and 19. 08:24 With adolescent idiopathic scoliosis, you will have greater progression in girls with boys. 08:30 It will start before menstruation. 08:34 You will have a low Risser sign. 08:36 We'll talk about a Risser sign and its relation to growth in just a minute. 08:40 You will most likely have double curves with the scoliosis starting in one area and being compensated for in another area. 08:48 It will be most likely starting in the thoracic spine. 08:51 The curves do get severe. It is important to measure the height of the person because they have the potential to lose height. 09:01 Congenital scoliosis is the second most common type of scoliosis after idiopathic. 09:06 These are generally progressive. 09:08 About three-quarters of congenital scoliosis will continue to worsen throughout life. 09:12 It can be associated with other congenital defects like cardiac defects or genitourinary defects. 09:19 In a congenital scoliosis, there is a specific vertebral defect. 09:25 Oftentimes, there's a failure to merge. 09:28 There's a failure of complete formation of the vertebrae. 09:31 You'll see hemivertebrae, wedge vertebrae, and segmentation, where you may have an open aspect of the vertebrae or incomplete formation. 09:41 So you have a failure of complete segmentation. 09:43 It's often unilateral. 09:46 It can be a bilateral failure as well or you can have a just open area in the back of the vertebrae. 09:53 It's also not uncommon to see fused ribs in a patient with a congenital scoliosis. 09:59 Another type of scoliosis is acquired scoliosis. 10:02 This is a person who has osteomalacia or had severe low back pain or had a psoas syndrome, could have had a broken leg or other fractures, they may have a hip prosthesis. 10:14 As a result of these abnormalities, you're going to have abnormal bone formation in other places. 10:22 Acquired scoliosis is something to pay attention to. 10:25 It happens and you will see it. 10:29 The most common causes of neuromusculoskeletal scoliosis are going to be a leg length discrepancy, neurofibromatosis, or quadriplegia. 10:37 When we look at neuromuscular scoliosis, there could be a neuropathy or it could be mesenchymal. 10:43 If you want to look at the most common causes of these, for neuropathy it's going to be cerebral palsy, Friedreich ataxia, myelomeningocele, spinal cord injury or others that are listed here. Of mesenchymal origin are the congenital defects like Ehlers–Danlos, homocystinuria and Marfan syndrome. 11:02 We can also talk about trauma related neuromuscular scoliosis which could be the direct vertebral trauma, extravertebral trauma. It could be a severe trunk burn or something that causes a thoracic injury and a loss of use of the body. 11:18 Irradiation is another possible traumatic cause. 11:21 In terms of tumor etiology of a neuromuscular scoliosis, you can have extramedullary effects like in a neurofibroma or intramedullary systems like an astrocytoma. 11:34 You could have an osteoid osteoma. 11:36 While rare, the osteoblastomas and bony tumors are a real cause of a scoliosis. 11:43 There are also myopathic causes. 11:45 You'll see that in arthrogryposis and other conditions listed here like Duchenne's muscular dystrophy, dysautonomia and the hyperphosphatemia issues, hypervitaminosis A. 11:56 So here's the list of the myopathic related neuromusculoskeletal issues causing scoliosis. 12:03 Then there are miscellaneous causes. 12:05 It is very common to see Charcot–Marie–Tooth causing a scoliosis as well as osteogenesis imperfecta, the blue sclera disease, and the soft bone disease. 12:17 Poliomyelitis which we no longer see or rickets are also possible causes of scoliosis. 12:23 So the list is noted here. 12:26 We will classify the scoliosis based on location. 12:29 Again, scoliosis will often have a double curvature. 12:34 We name it from the top of the curvature and the first vertebrae. 12:38 We name it based on the convexity. 12:43 Most frequent type of scoliosis is going to be thoracic and lumbar. 12:47 There'll be balanced curves with the thoracic and lumbar going in opposite directions. 12:52 You will have a crossover region which is a dangerous region because that's where you can have deterioration and degeneration of the vertebrae. 13:01 You can have a single thoracic scoliosis. 13:04 The progression in this kind of scoliosis can be damaging to the heart and lungs as well. 13:12 A single lumbar scoliosis also occurs. 13:15 That's associated with severe arthritic changes and lots of pain as well. 13:21 A junctional thoracolumbar scoliosis is also one that can occur. 13:24 You'll have a longer curve with that. 13:27 It over stresses the spine and causes arthritic changes in area of greatest pressure on the spine as well.
About the Lecture
The lecture Classifications of Scoliosis by Tyler Cymet, DO, FACOFP is from the course Osteopathic Treatment and Clinical Application by Region. It contains the following chapters:
- Classifications of Scoliosis
- Classifications of Scoliosis – Location
Included Quiz Questions
Which of the following are often used in the classification for scoliosis? (Select all that apply.)
- Reversibility
- Severity (angle)
- Causes (underlying disease)
- Location
- Family history
What is the radiological measurement used to quantify the magnitude of spinal deformities such as scoliosis?
- Cobb angle
- Sacral angle
- Thoracic angle
- Thoracic lumbar angle
Which of the following is the most common cause of scoliosis?
- Idiopathic scoliosis
- Congenital scoliosis
- Trauma related scoliosis
- Acquired scoliosis
- Neuromuscular scoliosis
Author of lecture Classifications of Scoliosis

Tyler Cymet, DO, FACOFP
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
It seemed easy at the beginning of the video but as it progressed was a bit confusing ...not pointing any1 to have failed to put up .presentation was very good but yes ...maybe the topic is boring ... else i liked it .. thanx for the video atleast can define and classify it easily now ...
