Playlist
Show Playlist
Hide Playlist
Leukemia: Chronic Myelogenous Leukemia (CML) – White Blood Cell Pathology

-
Slides Leukemia White Blood Cell Pathology.pdf
-
Download Lecture Overview
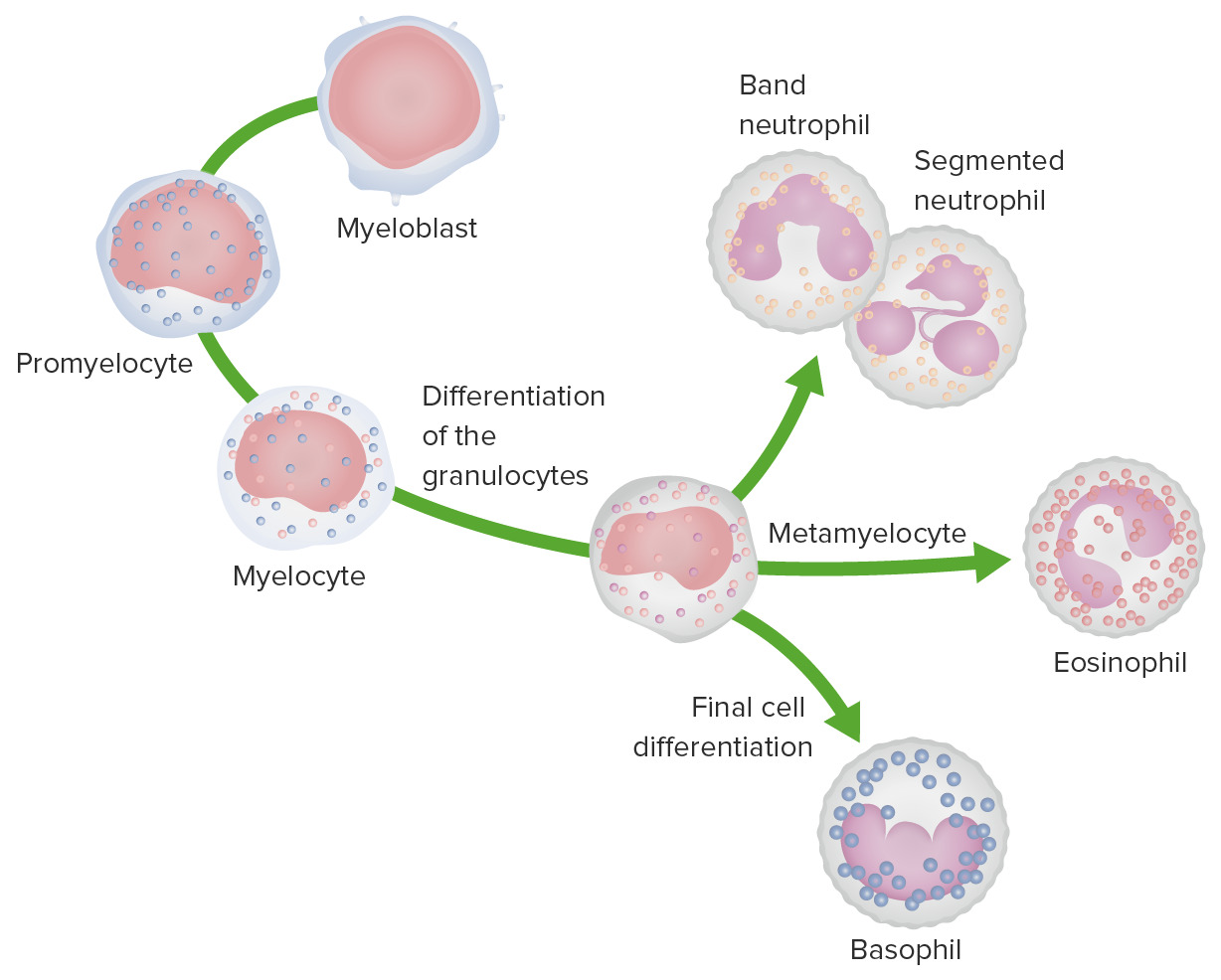
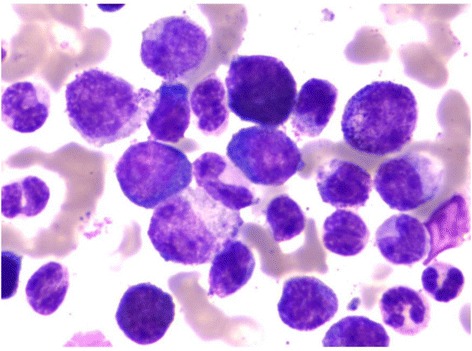
00:01 Let’s take a look at CML. 00:05 Here is the most important point. 00:07 Philadelphia chromosome translocation 9;22. 00:10 Genetically or molecularly, what is going to give rise to? It encodes for tyrosine kinase. 00:17 And you know that you can treat your 9;22 by giving your patient imatinib. 00:21 This is a fusion gene between BCR and ABL. 00:24 The ABL gene produces the tyrosine kinase. 00:27 And that’s important, important, important. 00:29 That is the target of the drug that you’re going to give this patient known as your imatinib. 00:35 The BCR/ABL fusion protein results in upregulation and so therefore, there is uncontrolled growth of this maturing myeloid cell. 00:42 So when you talk about chronic myelogenous leukemia, understand that technically this does come under your myeloproliferative disorders. 00:51 What does myeloproliferative mean? Your myeloid cells that are then increasing in number. 00:58 And when we get to that topic of myeloproliferative disorders We’ll be referring to what’s known as your polycythemia vera. 01:07 We’ll take a look at essential thrombocythemia, myelofibrosis. 01:10 And we’ll take a look at CML. 01:14 What’s going on with CML? Uh oh, translocation took place. 01:20 Fusion gene of your BCR/ABL. 01:23 What do you produce too much of? Good, tyrosine kinase. 01:27 What’s the name of that drug? Imatinib. 01:31 CML morphology. 01:32 What’re you going to find? On peripheral blood smear, you can expect to find increased numbers of mature myeloid cells. 01:40 However, you will be paying more attention to your basophilia. 01:45 Now you find immature granulocytes which you do not find these huge blasts. 01:49 Take a look at the picture here. 01:50 Do you find huge blasts in the picture? You can find immature granulocytes, I’ll give you that. 01:56 Such as myelocytes or metamyelocytes or bands, but you won’t find blasts. 02:01 Your focus should be on absolute basophilia. 02:04 What does that mean to you? That means that my WBC count is elevated and you find very high increase in basophils. 02:11 Remember, where is your basophil in the hierarchy? Basement. 02:20 Who is your patient? Forty-year-old, on average. 02:23 Insidious, not always true but in general correct. 02:29 Symptoms come from the anemia, splenomegaly, abdominal fullness. 02:34 So what’s this whole thing about me not being very, let’s say, confident about the insidious onset? It’s because they can have a really, really fast paced type of development. 02:49 And that is then called your blast crisis. 02:51 It’s important for us to pay attention in that in a second. 02:56 Diseases slowly progresses. 02:59 That’s what you are paying attention to. 03:01 An accelerated phase and the blast crisis. 03:06 Okay, now, it’s easy for me to say identical to AML but you’re the one taking the exam and obviously you’re going to ask me, "Well, how can I tell the difference? Well actually, it’s quite easy. 03:17 In AML, you know the basics, M0 to M7. 03:21 Say with different myeloid, FAB classification. 03:24 M3 gives you promyelocytic leukemia, give you translocation 15;17. 03:28 Gives you Auer rods. 03:29 You don't want to see that here in blast crisis. 03:32 What’s my topic? CML. 03:34 Speaking of CML, what’s the translocation here? Oh yeah, 9 and 22, tyrosine kinase, BCR/ABL. 03:41 Right? How old is your patient? Well, that part won’t help you too much, be careful. 03:46 And now, what are they going to go after? They’re going to make you think that, well, this student only knows about buzz words and I’m going to give my medical student a 40-year-old patient with leukemia and here, she is going to choose CML. 04:05 No, you’re not. 04:07 You’re going to be smart. 04:08 You’re going to rule things out accordingly and when you come to the answer choices, you knew to look for myeloperoxidase. 04:14 You knew to look for your translocation. 04:17 Maybe you find a gingival hyperplasia with M5 and you will confidently choose AML. 04:24 Or you went through this stem of question. 04:26 Patient was receiving imatinib and 9 and 22. 04:29 Oh, yeah, we have a blast count greater than 20% in the bone marrow. 04:34 Oh, this must be blast crisis of CML. 04:37 Right? Yes, that’s exactly what you’ll be doing. 04:41 You won’t miss a question on leukemia anymore. 04:46 CML and my drug is imatinib. 04:49 We talked about tyrosine kinase. 04:51 Yes, to confine resistance and that’s scary. 04:54 Look, cancer is behaving like infections. 04:58 You’ve heard of antibiotic resistance? Some of these cancers are so ridiculously intelligent that they actually will develop chemotherapy resistance. 05:08 At this point in your learning, you're left with no choice but bone marrow transplant, okay?
About the Lecture
The lecture Leukemia: Chronic Myelogenous Leukemia (CML) – White Blood Cell Pathology by Carlo Raj, MD is from the course Leukemia – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following translocations is associated with chronic myelogenous leukemia?
- t(9;22)
- t(11;14)
- t(15;17)
- t(8;21)
- t(14;18)
Which of the given enzymes is a product of the BCR-ABL fusion gene?
- Tyrosine kinase
- Thymidylate synthase
- Glutathione reductase
- Topoisomerase ii
- Thiamine oxidase
Which of the following drugs is used in the treatment of chronic myelogenous leukemia?
- Imatinib
- Lyrica
- Trazodone
- Adderall
- Amlodipine
Author of lecture Leukemia: Chronic Myelogenous Leukemia (CML) – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
So informative and well edited video , The Lecturer is excellent indeed .
I better understand CML. This was a very high yield lecture that was very well presented!
