Playlist
Show Playlist
Hide Playlist
Choledocholithiasis vs. Ascending Cholangitis with Case

-
Slides Gastroenterology 14 LBSD Gallstone Diseases.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
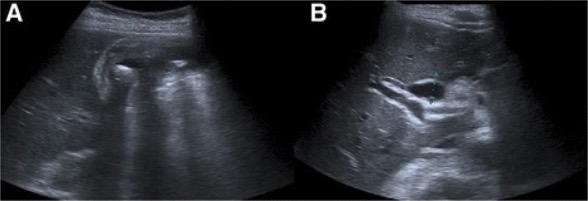
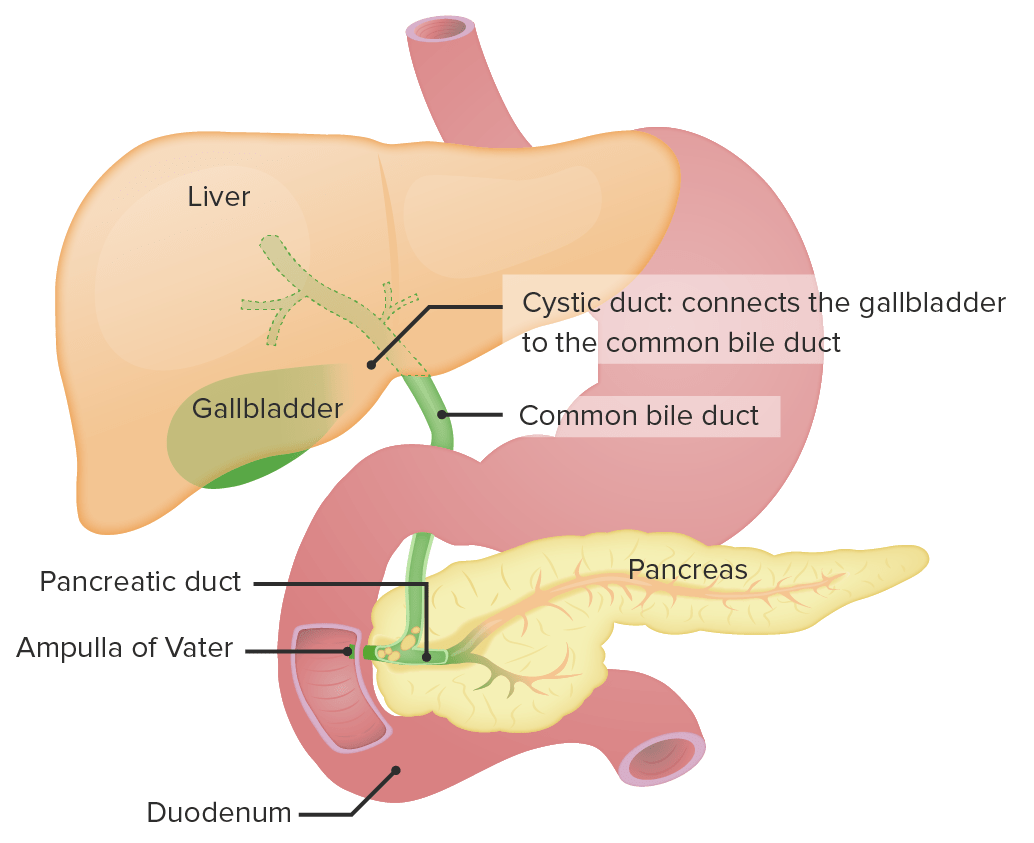
00:01 Let's move to our next case. 00:04 A 67-year-old woman is admitted to the hospital with 2 days of epigastric abdominal pain, fever and jaundice. 00:11 2 days ago, she had sudden onset abdominal pain then noticed her eyes and skin beginning to turn yellow. 00:18 Her vitals are notable for temperature of 39.3 C, blood pressure 105/58 (mmHg) and heart rate 105 (bpm). 00:26 Abdominal exam reveals right upper quadrant tenderness but no guarding. 00:30 Her labs are notable for a white cell count of 15,000/uL, ALT 550 (U/L) and total bilirubin of 7.2 (mg/dL) A right upper quadrant ultrasound shows dilated intrahepatic and extrahepatic bile ducts, gallstones, a normal gallbladder wall and no pericholecystic fluid. 00:51 So we are asked what is the recommended management? So let's point out that she has: epigastric pain, fever and jaundice - which is something called Charcot's triad She has fever, tachycardia and leukocytosis with a suspected biliary source given her elevated bilirubin and she meets criteria for sepsis. 01:15 And on imaging, she has dilated bile ducts with gallstones but none of those concerning findings for acute cholecystitis. 01:25 So let's talk again about choledocholithiasis. 01:28 Recall that this means the gallstone is now impacted in the common bile duct. 01:34 Patients will present very similarly to cholelithiasis. 01:40 They will often have a transient elevation in their serum AST, ALT, and bilirubin. 01:48 So, there are several complications that can occur. 01:51 Due to blockage of the common bile duct, you can develop an ascending infection, called cholangitis Or you may also develop gallstone pancreatitis. 02:02 The diagnosis is made by something called MRCP which is short for magnetic retrograde cholangiopancreatography. 02:10 An example is shown here. 02:17 You may also do right upper quadrant ultrasound which can detect ductal dilatation. 02:24 And treatment is with a procedure called an ERCP, this is endoscopic retrograde cholangiopancreatography This is a procedure by which we can remove the stone that's impacted in the common bile duct. 02:39 So, we mentioned the complication of gallstone pancreatitis. 02:42 This occurs when the gallstone is impacted in the common bile duct such that it also blocks the pancreatic duct. 02:50 When this happens, patients may develop pancreatitis. 02:55 We also mentioned the procedure called an ERCP. 02:58 Basically, what this looks like is a scope that is advanced into the duodenum and then we use a guide wire to insert through the sphincter of Odi into the common bile duct. 03:10 This guide wire could help us either do a sphincterotomy which means widening the sphincter to allow passage of the stone, or we can also remove the stone directly form the common bile duct. 03:24 So, patients may present with certain symptoms, that one of which we characterize as Charcot's triad. 03:31 This is a triad of symptoms of fever, right upper quadrant pain, and jaundice. 03:38 When the infection becomes more severe, they may develop what's called, Reynold's pentad. 03:44 This is when they have fever, right upper quadrant pain and jaundice, but also the addition of hypotension and altered mental status. 03:53 These are just two common eponyms that you should learn for test-taking purposes. 04:00 So now let's get to the management of this condition, If your diagnosis is unclear, you may do an MRCP or an endoscopic ultrasound to confirm the diagnosis if you don't already have that based on their ultrasound or CT imaging. 04:15 You may give supportive care with IV fluids And broad-spectrum IV antibiotics, again wanting to target the GI flora so gram negatives and anaerobes And lastly, you may then do an ERCP to remove the stone and perform a sphincterotomy. 04:34 Here on the right, you can see an example of an ERCP image. 04:38 That arrow indicates a small darkened area within the common bile duct. 04:42 That is a gallstone impacted. 04:47 So now, let's return to our case. 04:49 A 67-year-old woman with epigastric abdominal pain, fever and jaundice which is Charcot's triad for cholangitis. 04:57 She has signs of sepsis with a suspected biliary source and on imaging, she has dilated bile ducts but no signs of acute cholecystitis. 05:06 So, we now know that the presence of the dilated bile ducts with Charcot's triad of symptoms, in the case that she likely has a stone impacted in the common bile duct leading to ascending cholangitis. 05:19 So the recommended management would be supportive care with IV antibiotics and then ERCP to disimpact the common bile duct.
About the Lecture
The lecture Choledocholithiasis vs. Ascending Cholangitis with Case by Kelley Chuang, MD is from the course Disorders of the Hepatobiliary Tract.
Included Quiz Questions
Which of the following is the treatment of choice for choledocholithiasis?
- ERCP
- MRCP
- Ceftriaxone
- Proton pump inhibitors
- Metronidazole
Which of the following clinical manifestations is part of the Charcot triad?
- Jaundice
- Hypotension
- Altered mental status
- Dizziness
- Diffuse abdominal pain
What is the best way to confirm the presence of ascending cholangitis if the abdominal ultrasound or CT findings are equivocal?
- Endoscopic ultrasound or MRCP
- Colonoscopy
- Abdominal MRI
- Paracentesis
- Endoscopy
Author of lecture Choledocholithiasis vs. Ascending Cholangitis with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
