Playlist
Show Playlist
Hide Playlist
Cholangiocarcinoma with Case

-
Slides Gastroenterology 17 Hepatobiliary Malignancy.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
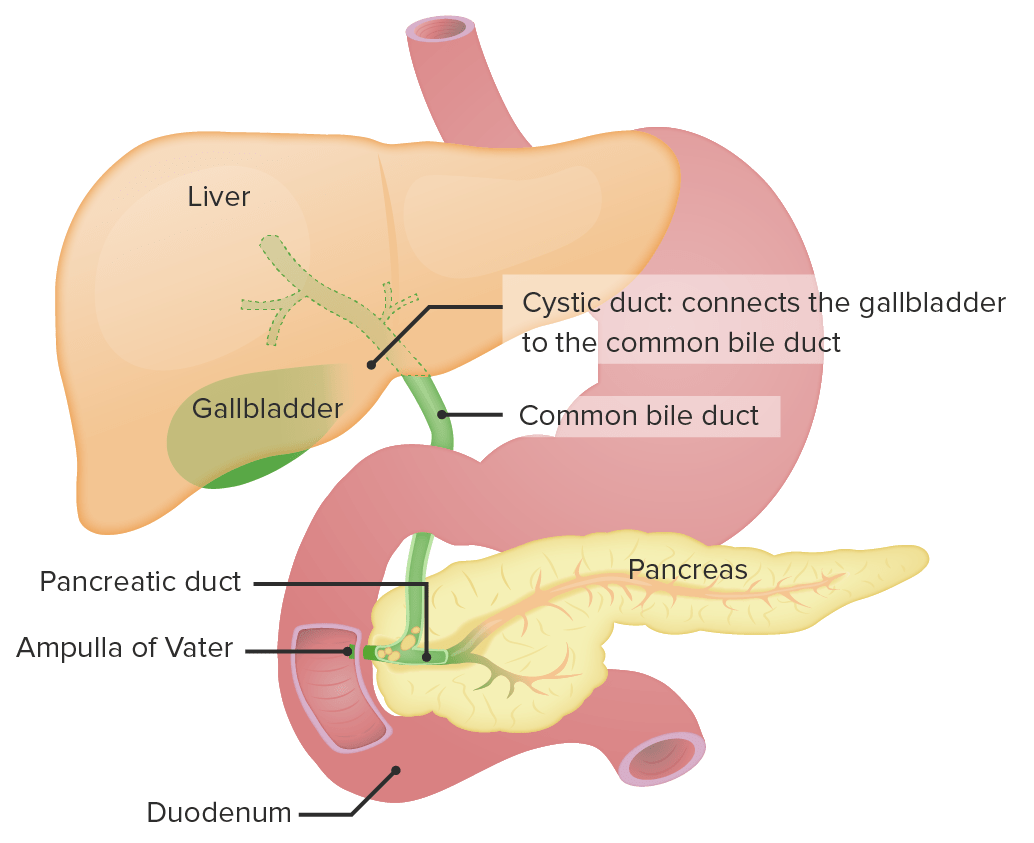
00:02 Let's move on to our next case. 00:04 A 68-year-old woman with a history of primary sclerosing cholangitis presents to her primary care physician with 3 months of jaundice, weight loss and abdominal pain. 00:15 She has had a dull ache in her right upper quadrant for the past few months. 00:20 Vitals are normal. 00:21 Physical exam reveals jaundice, scleral icterus, diffuse muscle wasting and tenderness to palpation in the right upper quadrant. 00:29 Her lab studies are notable for AST of 99 (U/L), ALT 89 (U/L), total bilirubin 8.2 (mg/dL) and alkaline phosphatase 89 (U/L). 00:39 A serum CA19-9 is elevated. 00:42 An abdominal ultrasound shows a dilated intra and extrahepatic bile ducts, hepatomegaly but no obvious hepatic masses. 00:50 What is the best next step to confirm the diagnosis? So let's point out some key things here. 00:57 She has jaundice, weight loss and right upper quadrant pain and know that she has a history of PSC. 01:04 Her physical exam and lab findings are consistent with a cholestatic picture leading to jaundice. 01:11 And we're told that she has an elevated CA19-9 which is a type of tumor marker, with dilated biliary ducts. 01:19 So, those may be clues to help us figure out the diagnosis. 01:24 So now let's speak a bit about cholangiocarcinoma. 01:27 This is a cancer that is specific to the bile duct. 01:31 It can originate anywhere along the biliary system so it can be intrahepatic - within the liver, or along the extrahepatic ducts - outside of the liver. 01:43 It is the second most common primary cancer of the liver after HCC, and patients may come in with right upper quadrant pain. 01:51 They may have constitutional symptoms of generalized fatigue, and weight loss and they may have jaundice. 01:59 The diagnosis is mostly by imaging which can be done with MRCP or CT scan. 02:06 In addition, in unclear cases, you might do an ERCP and take brushings of the bile duct or biopsy to help you confirm the diagnosis. 02:16 A serum CA 19-9 is a tumor marker that you can check, which may be elevated but know that this cannot help you confirm or exclude the diagnosis. 02:28 Where it can be helpful, is in tracking response to treatment and whether or not patients have experienced remission or relapse. 02:38 So there are several risk factors for cholangiocarcinoma. 02:41 The first one, is a history of primary sclerosing cholangitis. 02:46 Patients who have choledochal cysts may also be at risk. 02:49 Rarely, liver fluke infections can cause this cancer. 02:54 They may have prior exposure to thorium dioxide and stones within the liver, so hepatolithiasis can also predispose patients to this condition. 03:06 So the treatment depends on how extensive the disease is. 03:11 Usually, if the disease is limited to the distal bile ducts outside of the liver, you may do surgical resection. 03:18 For those lesions that are non-resectable, either they involve structures around the biliary tree and have invaded elsewhere, you may do chemotherapy. 03:29 For those patients who then develop obstruction from the cancer itself of the bile duct, we may offer endoscopic stenting. 03:37 So here you can see first an example of an MRCP showing a stricture in the bile duct, And panel B, you now know see an ERCP with a scope that has been advanced and this is prior to stenting. 03:51 And in panel C, you now see a stent being placed and adequate flow through the biliary tree. 03:59 Lastly, the last treatment option we have is liver transplantation when disease is non-resectable, if it is less than 3 cm in size and has not spread beyond the liver. 04:13 So, unfortunately, cholangiocarcinoma is often a fatal diagnosis. 04:18 By the time most patient presents, because they have such a vague symptoms, they often have disease that is no longer resectable. 04:27 So now, let's return to our case. 04:29 Our 68-year-old woman with a history of PSC, is now coming in with jaundice and weight loss, as well as right upper quadrant pain. 04:37 Her physical exam and labs are consistent with a cholestatic picture and her elevated CA19-9 is a hint that there may be something going on related to malignancy. 04:48 So, that in addition to her bile ducts on the ultrasound should make you suspicious for cholangiocarcinoma, and the best next step to confirm the diagnosis is an ERCP for the biopsy to confirm.
About the Lecture
The lecture Cholangiocarcinoma with Case by Kelley Chuang, MD is from the course Disorders of the Hepatobiliary Tract.
Included Quiz Questions
Which of the following medical conditions is the most significant risk factor for cholangiocarcinoma?
- Primary sclerosing cholangitis
- Viral hepatitis
- Primary biliary cholangitis
- Hemochromatosis
- Autoimmune hepatitis
Which of the following is the treatment of choice for cholangiocarcinoma limited to the distal bile ducts outside of the liver?
- Surgical resection
- Chemotherapy
- Liver transplantation
- Endoscopic stenting
- Radiation
Which of the following is the test of choice for the confirmation of cholangiocarcinoma?
- ERCP with biopsy
- Serum CA 19-9
- Abdominal ultrasonography
- Abdominal CT
- Colonoscopy
Author of lecture Cholangiocarcinoma with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
