Playlist
Show Playlist
Hide Playlist
Chlamydia Trachomatis

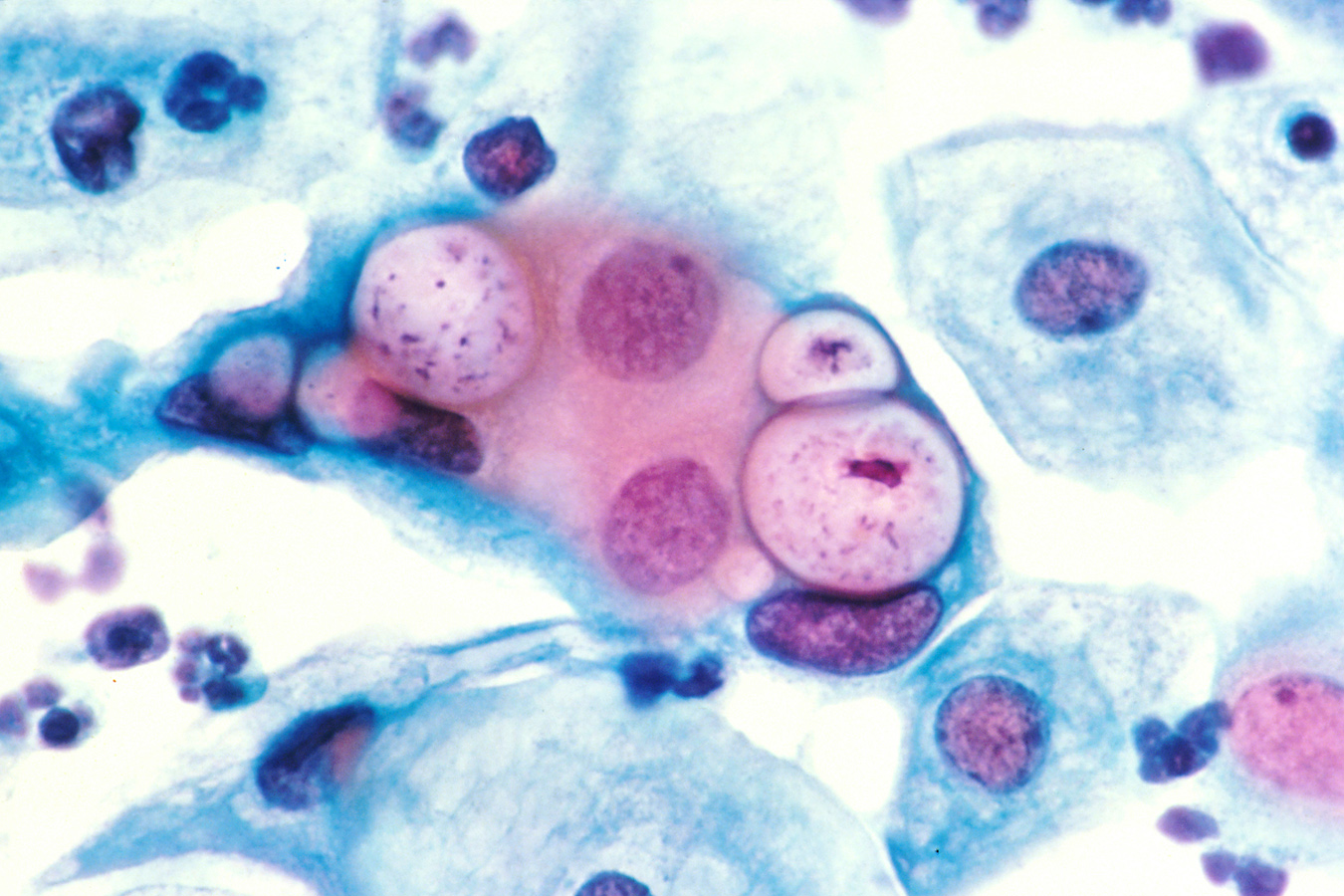
00:01 Identification then specific again to Chlamydia Trachomatis. 00:05 The iodine-staining of the inclusion bodies is very, very specific. 00:10 However, it is not that sensitive. 00:13 One would have to capture a certain number of cells all at the stage of showing inclusion bodies to be able to see or visualize presence of that positive stain. 00:23 One can also grow and isolate in cell culture but far more often, we’re making a diagnosis of Chlamydia Trachomatis by molecular diagnostics using PCR on urine specimens or on genital swabs. 00:37 In addition, we can look for Chlamydial antigens and nucleic acid sequences. 00:42 Then, of course, there are serologic conversions, development of immunoglobulin M and immunoglobulin G to specific antigens expressed by the Chlamydia creating anti-Chlamydial antibodies. 00:57 So, mechanisms of pathogenesis. 01:00 If we now look for types A through K of the Chlamydia Trachomatis, it binds itself to the non-ciliated epithelial cells of mucous membranes via the elementary body binding receptors on the cell’s surface. 01:15 Those cells, those target cells can be found in many, many, many places but especially in the urethra, the vagina, fallopian tubes, anorectal tract, again, going along with the sexually transmitted nature but also, can be found in the respiratory tract and in the conjunctiva. 01:33 Types L1, 2 and 3 with Chlamydia Trachomatis will typically bind to macrophages, again, via specific receptor and then, internalization of phagocytosis. 01:47 As they replicate in their inclusion body however, the target cell, the target macrophage ultimately is destroyed. 01:55 It is the destruction of the target cells and then, the exposure to the host immune system which ultimately finally drives disease manifestations and this is a recurring theme with many of these very small intracellular organisms in that disease or clinical signs don’t truly manifest until there’s exposure outside the host cell. 02:20 Looking then back to Chlamydia Trachomatis types L1 to L3, we’re going to look at how and why, and what they do in the various forms of infection which they occur. 02:33 The three principal infections we’ll look at are urogenital infections, systemic infections, and ocular or ophthalmologic infections. 02:43 Transmission of the first two, the urogenital and systemic infections is via sexual exposure, sexual contact and this is where the principal infection occurs. 02:53 Ocular infections then typically occur through autoinoculation typically by the hands, the fingers which become contaminated potentially while going to the toilet or cleaning up after intercourse and then, autoinoculating or transferring active, infective organism to the conjunctiva, to the eye. 03:14 Ocular genital contact also can occur through other types of vector transmission or Kleenex, tissue, etc. 03:23 The presentation then for urogenital infections after sexual contact has occurred in women, typically is a cervicitis, urethritis, or salpingitis. 03:35 Some people wrap these all together into pelvic inflammatory disease but just basically think of this as inflammation or itis of any part of the women’s reproductive tract. 03:46 In men, the itis or inflammation similarly occurs along the genitalia, including the urethra, the epididymitis, the prostate and around the anus. 03:57 As that infection or if that infection becomes systemic, if it generalizes, women will further develop a post-infectious inflammatory arthritis and dermatitis. 04:10 Men will develop Reiter’s syndrome which we’ll describe in just a second or two. 04:15 Ocular infections are in adult, the inclusion conjunctivitis which are best seen by an ophthalmologist with a slit lamp examination. 04:25 Further on, clinical manifestations after the presentation, in the women, they may have asymptomatic infection. 04:33 In fact, many of the inflammatory processes are silent or clinically non-discoverable. 04:40 Symptomatic infections only develop when mucopurulent discharge is expressed or the patient has clinical symptoms of dysuria, painful urination, or pyuria, some sort of other purulent discharge elsewhere. 04:55 The Reiter syndrome that we just described for men especially who have systemic progression of their Chlamydia Trachomatis infection is a classic triad of arthritis, urethritis, and uveitis. 05:08 It is most often a post-infectious, an immunologic reaction to antigens expressed by the Chlamydia Trachomatis. 05:16 In the ocular setting, the clinical manifestations of the adult inclusion conjunctivitis are a mucopurulent discharge of course, along with keratitis or inflammation of the sclera, the cornea, with high potential for scarring after on. Looking at neonatal infections. 05:34 These are a direct offshoot of sexually acquired infections by the mother and then, passage through to the baby most often during delivery. 05:44 So, as the baby’s delivered through, typically, it’s the presenting part of the baby that the head, the eyes, the nose, which are first exposed and potentially, first infected with Chlamydia Trachomatis, thus, neonatal infection most often is seen as neonatal conjunctivitis and in this case, the infants will develop slow onset of mucopurulent discharge from their conjunctivae beginning at two days of life up to even a full 30 days or so. 06:15 The swelling of the eyelids is associated with this as is a very purulent discharge and if this is not recognized and not treated, then, corneal vascularization or neovascularization can occur and followed by conjunctival scarring. 06:32 Prevention for this possibility is typically encountered by providing topical erythromycin ointment to the eyes. 06:40 Why do we even need to worry about this? Well, remember again that I said that many of the female sexually acquired Chlamydia infections are silent. 06:50 They’re not clinically evident. 06:52 So, a baby could be born to and exposed to a Chlamydia infected mother without any suspicion by the healthcare provider, thus, topical erythromycin is a routine practice for postpartum or post-delivery infants around the world. 07:07 Infant pneumonia with Chlamydia Trachomatis is a secondary process which is acquired by the infant swallowing or aspirating genital secretions contaminated with Chlamydia Trachomatis. 07:22 It’s very important to distinguish infant pneumonia caused by Chlamydia Trachomatis from pneumonia caused by Chlamydia Pneumoniae, a separate organism which we’ll talk about in just a little bit. 07:33 Chlamydia Pneumoniae as a cause of pneumonia can affect anybody. 07:38 We’re talking in this case specific about babies exposed to Chlamydia Trachomatis who then develop a pneumonia caused by that organism. 07:47 When they do so, it occurs two to three weeks after delivery and it is associated with upper and lower respiratory tract infection signs, especially a clear rhinitis, a clear nasal discharge, and then a staccato cough, discrete individual coughs, not paroxysmal cough such as you might see with Pertussis or whooping cough. 08:08 So, individual coughs, cough, cough, cough, and very importantly, these infants don’t have fever. 08:16 In fact, many times, this diagnosis is made by accident when a chest x-ray is performed looking for some other cause of the cough, perhaps, an aspirated foreign object or perhaps something else like a virus. 08:30 When the x-ray is performed however and as you can see in the lower right part of the slide, it shows diffuse interstitial pneumonia throughout the lung fields. 08:41 Many times, the x-rays are described as white patches throughout all of the lung fields. 08:47 Now, let’s go to some of the other very exciting sexually acquired forms of Chlamydia Trachomatis types D through K and here, we’re looking specifically at lymphogranuloma venereum. 09:00 This is as you can imagine acquired through sexual contact and there are two different stages for this process. 09:07 The first or initial stage occurs roughly a month to up till six weeks after exposure to the Chlamydia Trachomatis and patients develop a small painless lesion at the site of the inoculation. 09:22 This may be the glans penis, this may be somewhere around the vaginal introitus and it is typically associated with low grade fever, headaches, and myalgias. 09:32 This yet still believe it or not be an asymptomatic presentation if the patient does not notice the lesion. 09:40 Again, it’s painless so they may not notice it at all and they may simply think that they had some routine virus, the flu or something like that. 09:48 However, after the resolution of this stage, the late stage develops and this is draining purulent discharge from a sinus tract from the lymph nodes. 10:00 In fact, most inguinal lymph nodes in the bilateral region will become enlarged, will become painful, they’ll develop fistulas, and even local ulcers. 10:12 This of course is quite symptomatic and quite noticeable to patients and this is typically the stage at which they come to medical attention. 10:20 When they do so, doxycycline is the drug of choice as it treats most of the unusual or atypical sexually transmitted infections including especially Chlamydia Trachomatis types D through K. 10:32 There are ocular manifestations of Chlamydia Trachomatis as well and these are transmitted through infected tears as well as hand to eye or auto-transmission of infected materials, clothing, Kleenex, etc. and so forth. 10:50 This is unfortunately an incredibly significant problem in parts of the world which are underserved and especially in Africa and it is known as a leading cause of preventable blindness. 11:04 Again, as with the sexually transmitted infection we just talked about, this occurs in two stages. 11:11 The first stage is a follicular conjunctivitis such as you see in the two pictures to the left side of the screen. 11:19 You can see prominent blood vessels of the under aspect of the eyelid and the conjunctiva itself in the third picture from the left shows prominent conjunctival vessels. 11:32 This stage is associated with pain, photophobia and increased tearing, lacrimation. 11:38 The late stage occurring weeks to months afterwards then progresses to a very hard fixed organized inflammatory reaction in which the papillae become firm, in fact, rock hard erythematous and the eyelids involute or turn in as you see in the far picture on the right. 11:57 This then because of physical trauma leads to corneal abrasion, followed by ulceration, followed by scarring, and eventually, blindness. 12:08 Again, preventable if the infection were diagnosed and treated in the early stages and again, a tetracycline would be the way to go. 12:16 Overall, prevention and treatment, safe sex practices, barrier contraception, seeking care when somebody is infected or may be infected, improved personal hygiene and by this, I mean to try and prevent the autoinoculation via the hands, using hand hygiene in terms of alcohol-based hand cleaners, soap and water, all those will be very effective in preventing or at least limiting the impact of autoinoculation. 12:44 Treatment for all the chlamydia infections even though I just told you doxycycline is actually azithromycin. 12:51 It’s preferred because a single large dose of azithromycin is both curative as well as easy to administer. 13:01 The only problem is that single large dose of azithromycin is not very well tolerated and in many third world parts of the world, it is not even available, and so, doxycycline is a go-to antibiotic as well. 13:16 So, that summarizes what we know about Chlamydia Trachomatis and it’s really just scratching the surface of the devastation which can be caused by that sexually transmitted infection.
About the Lecture
The lecture Chlamydia Trachomatis by Sean Elliott, MD is from the course Bacteria.
Included Quiz Questions
What type of stain is used to identify Chlamydia trachomatis?
- Iodine stain
- Silver stain
- Gram stain
- Romanowsky stain
- PAS stain
Which system of the body is the most common target of Chlamydia trachomatis?
- Genitourinary system
- Gastrointestinal system
- Respiratory system
- Integumentary system
- Cardiovascular system
In female patients, what is the presentation of urogenital infection caused by Chlamydia trachomatis?
- Urethritis, salpingitis, and cervicitis
- Urethritis, appendicitis, and salpingitis
- Cervicitis, urethritis, and gastritis
- Appendicitis, salpingitis, and gastritis
- Urethritis, salpingitis, and gastritis
Which type of ocular infection is caused by Chlamydia trachomatis in adults?
- Conjunctivitis
- Blepharitis
- Keratoconjunctivitis
- Keratitis
- Endophthalmitis
Which of the following represents the classic triad of reactive arthritis?
- Arthritis, urethritis, and uveitis
- Arthritis, blepharitis, and uveitis
- Urethritis, vaginitis, and arthritis
- Arthritis, uveitis, and vaginitis
- Vaginitis, blepharitis, and arthritis
Which of the following neonatal infection(s) can be caused by Chlamydia trachomatis after 2 days up to 30 days after birth? Select all that apply.
- Pneumonia
- Dermatitis
- Bronchitis
- Asthma
- Conjunctivitis
What is the drug of choice for lymphogranuloma venereum caused by Chlamydia trachomatis?
- Doxycycline
- Gentamicin
- Penicillin
- Ceftriaxone
- Ampicillin
Author of lecture Chlamydia Trachomatis

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
