Playlist
Show Playlist
Hide Playlist
Chest Abnormalities in Pediatric Radiology

-
Slides Pediatric Chest.pdf
-
Download Lecture Overview
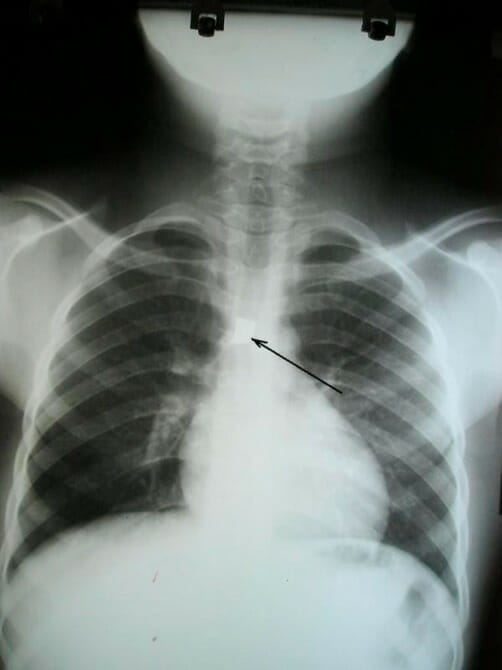
00:01 So in this lecture, I'd like to review some commonly encountered chest abnormalities within the neonatal and pediatric population. 00:07 This can differ significantly from adult chest disease and so let's take a look at some of the commonly encountered findings. 00:13 We'll start off with the neonatal period. 00:16 So the three most commonly encountered abnormalities in the neonatal period include transient tachypnea of the newborn, meconium aspiration syndrome and hyaline membrane disease. 00:27 With transient tachypnea of the newborn, this is caused by delayed clearance of fetal pulmonary fluid. 00:33 This is actually more commonly seen in babies that are delivered by c-section because of lack of the thoracic squeeze that normally occurs during vaginal delivery. 00:41 So the thought is that during vaginal delivery, the thorax is squeezed, squeezing out extrapulmonary fluid. 00:48 However, babies that are delivered by c-section don't go through the vagina and don't have this thoracic squeeze, and so they actually have a harder time clearing out their pulmonary fluid that's residual in their lungs. 00:58 This can also be seen after patients that undergo short labor or in infants of mothers with diabetes. 01:05 So imaging findings are similar to that of fluid overload. 01:09 So it appears similar to what we would see in pulmonary edema. 01:12 You have hazy pulmonary vasculature, so ground glass appearance to the lungs. 01:17 The heart looks like it's enlarged and you may have fluid in the fissures as pointed out by the white arrow. 01:23 You can also have small pleural effusions. 01:25 We can see a small one on the right here that's pointed out by the black arrow. 01:28 Both lungs here have a hazy ground glass appearance which is commonly seen. 01:34 Meconium Aspiration Syndrome occurs from aspiration of meconium just prior to or during delivery. 01:40 This occurs more commonly in babies that are delivered at a very late gestational stage and it can cause obstruction of the small airways and it can actually result in a chemical pneumonitis. 01:50 These can actually result in a severe respiratory failure. 01:53 So as you can see here, the lungs appear very hyperinflated which is commonly seen with meconium aspiration syndrome. 01:58 You can also see ropy perihilar opacities and you can see patchy areas of consolidation, so here if you look in the perihilar region, you can see what appear to be these ropy opacities in both lungs. 02:11 You can also see an area of consolidation that silhouettes the right hemidiaphragm. 02:16 This can actually result in pneumothorax, so it's important to take a look at these chest x-rays to make sure there isn't the presence of a pneumothorax which if large enough can lead to cardiopulmonary collapse. 02:26 Hyaline Membrane Disease is also called surfactant-deficiency disease or respiratory distress syndrome. 02:31 This is caused by the inability of the pneumocytes to produce surfactant and without surfactant the alveoli collapse and result in atelectasis of the lungs. 02:40 This is most commonly seen in very premature infants that are born at less than 34 weeks of gestation and it's the leading cause of death in newborns. 02:48 So this is an example of a patient with Hyaline Membrane Disease. 02:52 In this case, you could see that the lung volumes are actually low and again as with some of the other abnormalities, you can see a diffused granular or ground glass appearance to both lungs. 03:01 With Hyaline Membrane Disease, you may also have the presence of air bronchograms. 03:07 Let's move on to common childhood airway diseases. 03:10 This includes reactive airway disease which is very commonly seen in kids. 03:15 This is a general process that presents in the pediatric population and it results in wheezing, shortness of breath and coughing presenting clinically. 03:22 This is usually transient but often it can progress on to asthma. 03:26 With reactive airway disease, we can actually see the walls of the bronchi in the perihilar region and this is due to the perihilar peribronchial thickening. 03:34 So you can see here pointed out by the arrows. 03:36 You can see the loosened bronchi and then you can see the thickening of the wall around them. 03:42 This can actually appear like donuts in the perihilar region. 03:45 The patients have also hyperinflated lungs and they have a significant amount of mucus plugging which can result in atelectasis. 03:52 Epiglottitis is another relatively commonly seen airway disease. 03:57 It's actually becoming somewhat less in frequency these days but if when it does present, it can be life-threatening. 04:02 It usually presents in kids that are between the ages of 3 and 6 and it's an infection causing edema of the epiglottis. 04:09 This can result in airway obstruction which is why it becomes life threatening very quickly. 04:14 Common causes include infection with h. flu type B and is preventable by immunization which is why the incidence is actually decreased overtime. 04:22 This is most commonly and most quickly diagnosed by a lateral radiograph of the neck. 04:26 Clinically, patients present with stridor, drooling, dysphagia and fever, so whenever a patient presents with stridor, you always wanna make sure that there isn't an obstructive lesion of the neck and epiglottis in a patient that has both stridor and fever is one of the things that you wanna think about. 04:42 So you can see here 2 lateral images of the neck. 04:46 The left image demonstrates a normal epiglottis and you can see that pointed out by the arrow. 04:51 The right image is a patient that has epiglottitis which you can also see pointed out by the arrow and if you take a look at the difference, the epiglottis in a normal patient is a very thin structure while in a patient with epiglottitis, it's a much thicker structure which can result in obstruction of the airway. 05:08 In a patient that has epiglottitis, the epiglottis has a "thumb-like" appearance. 05:13 So let's discuss croup. 05:15 Croup is most commonly caused by parainfluenza virus and it occurs usually between the ages of 6 months and 3 years. 05:22 The most common clinical symptom is a barking cough which sounds very different than regular cough and once you've heard it, it's very easy to recognize again. 05:30 These are usually diagnosed clinically because of the very classic barking cough. 05:35 However, you can obtain a radiograph just to exclude other causes of airway obstruction. 05:40 It's usually diagnosed with a frontal and a lateral radiograph and you can see here on the frontal view, the airway has an upside down "V" appearance which is also called the "steeple sign." On the lateral radiograph, you have narrowing of the subglottic trachea which is outlined here by the arrow and you have distention of the hypopharynx. 06:01 So because you have a narrowing distally, you have a dilatation more anteriorly of the pharynx. 06:08 Again, this is somewhat of a classic radiographic sign, it's not always seen in patients and that's why patients are usually diagnosed just with that barking cough that they present with. 06:17 Aspirated foreign body is something very important to recognize in a kid. 06:21 So aspirated foreign bodies often lodge within the bronchus and a standard inspiratory radiograph may be normal. 06:27 So in suspected cases of aspiration, you wanna perform both an inspiratory and an expiratory film to take a better look at the airway In children who can't cooperate with inspiration and expiration, you can perform bilateral decubitus fuse. 06:40 So let's take a look at this case. 06:43 This patient has a suspected foreign body. 06:46 Which side do you think is abnormal? You see on this frontal radiograph, there are asymmetric lung volumes. 06:52 The lung volume is increased on the right and it's decreased on the left and it's hard really to determine which one is abnormal. 07:05 So in this patient we performed bilateral decubitus fuse because the patient was too young to cooperate with inspiration and expiration. 07:11 So the image on the left is done with the right side of the patient down and then the image on the right is done with the left side of the patient down. 07:20 So now, can you tell which one is abnormal? So this actually demonstrates that the right lateral decubitus film shows no change in volume of the right lung. 07:35 So this is the right lung here. 07:37 Generally, because of gravity the lung that is in the lower position should decompress and if it doesn't and it remains persistently hyperinflated, that's the side of the abnormality. 07:48 The left decubitus film demonstrate normal collapse of the left lung in this position. 07:53 So this is what you would normally expect to see. 07:56 The lung that's again in the lower position should collapse because of the gravity, so this imaging indicates there is obstruction of the right mainstem bronchus with a foreign body. 08:04 So this patient ended up having a bronchoscopy to remove the foreign body that was lodged in there. 08:09 So we've gone over some common abnormalities that you might encounter in the neonatal period and in kids. 08:14 Again, very different than what you might encounter in an adult.
About the Lecture
The lecture Chest Abnormalities in Pediatric Radiology by Hetal Verma, MD is from the course Pediatric Radiology. It contains the following chapters:
- Chest Abnormalities
- Common Childhood Airways Disease
Included Quiz Questions
What is TRUE regarding hyaline membrane disease in an infant?
- It is caused by the inability of pneumocytes to produce surfactant.
- It is seen more commonly in babies delivered by C-section.
- It is more often seen in infants delivered at a late gestational stage.
- Imaging findings are similar to those of fluid overload.
- Pleural effusions are commonly seen.
Which of the following is a complication of meconium aspiration syndrome?
- Pneumothorax
- Pleural effusion
- Cardiomegaly
- Renal failure
- Surfactant deficiency
Perihilar bronchial thickening is seen on a chest X-ray of a 5-year-old child presenting with shortness of breath. Which of the following is the most likely diagnosis?
- Reactive airway disease
- Hyaline membrane disease
- Transient tachypnea of the child
- Meconium aspiration syndrome
- Pneumonia
Which of the following is a life-threatening infection in a child leading to airway obstruction?
- Epiglottitis
- Pneumonia
- Asthma
- Hyaline membrane disease
- Reactive airway disease
Author of lecture Chest Abnormalities in Pediatric Radiology

Hetal Verma, MD
Customer reviews
3,7 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
she focus on her specalty, what you need to know about pediatric ragiology
Good overview, hits on most important images. More detail about physiology behind why images present as such would have been good.
she reads everything from the slides ....her courses are really boring
