Playlist
Show Playlist
Hide Playlist
Chancroid: Diagnosis and Therapy


-
Slides Chancroid InfectiousDiseases.pdf
-
Reference List Infectious Diseases.pdf
-
Download Lecture Overview
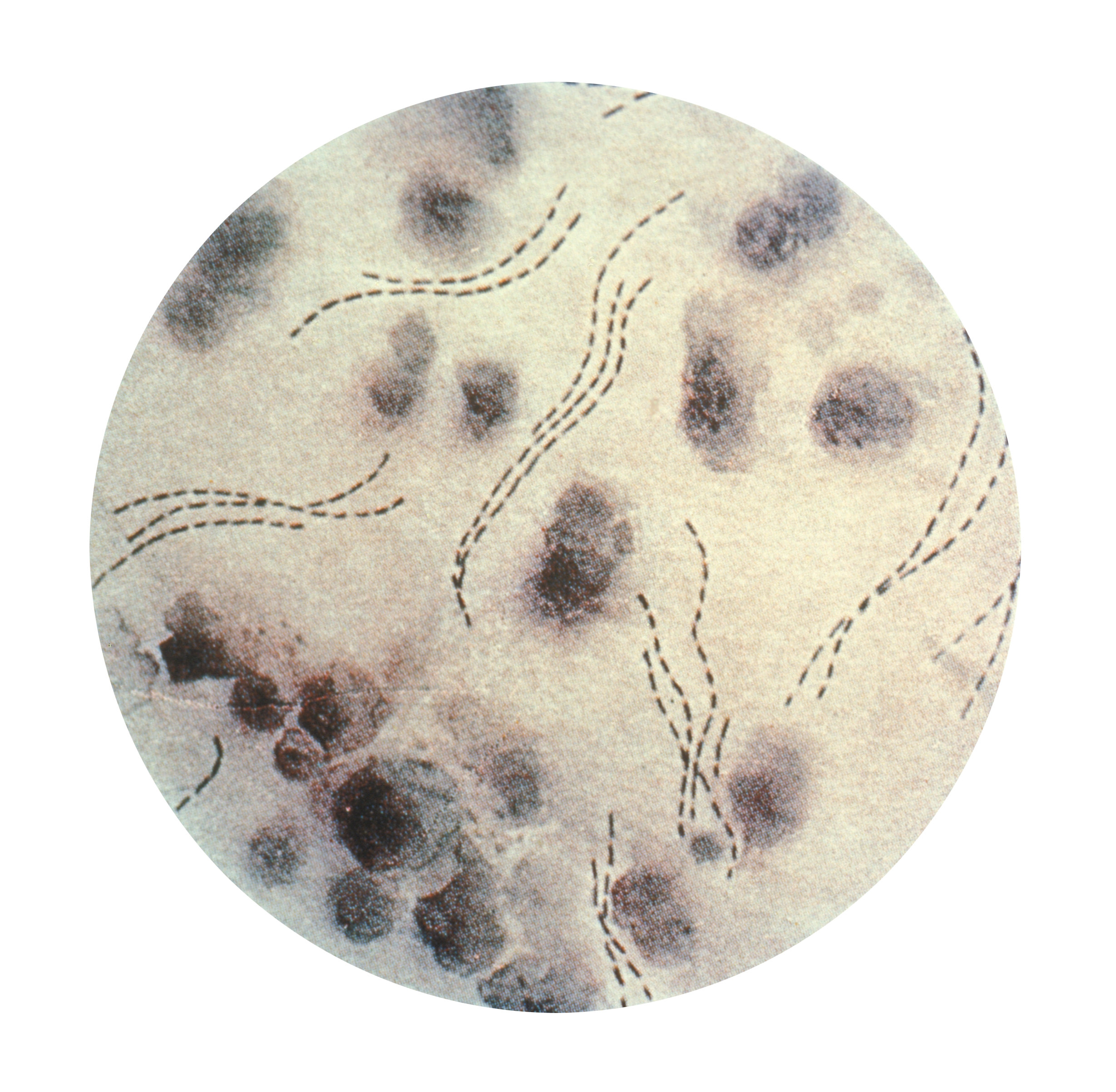
00:01 You make a diagnosis of definite chancroid by detecting antigens of Haemophilus ducreyi by PCR. 00:14 that’s the way to make them. 00:16 Gram stain is not that sensitive. 00:22 It’s probable chancroid if a patient presents with one or more genital ulcers that are painful, and you’ve ruled out syphilis – no evidence of Treponema pallidum either by dark field, or their serology is negative. 00:39 Or if they have a typical clinical presentation, and you’ve also thought about herpes simplex and you’ve tested for that, and the test for herpes simplex is negative – that would be examples of probable chancroid. 00:57 Now in terms of treatment, azithromycin in a single dose is very effective. 01:07 Alternatives include ceftriaxone, a single intramuscular dose, and remember that this is a Gram-negative pleomorphic rod, and like ceftriaxone works with Haemophilus influenzae. 01:24 You wouldn’t be surprised that it also works for Haemophilus ducreyi. 01:29 Ditto ciprofloxacin given for 3 days and erythromycin given for 7 days. 01:37 And what you would expect in a patient is that they would be better in 3-7 days. 01:43 If they’re not better, then perhaps the diagnosis is not correct. 01:48 So what do we do about a patient who you thought had chancroid but you weren’t able to prove it and they didn’t get any better? Well the main thing that you want to rule out is the painful genital infection due to herpes simplex, and also an atypical presentation of primary syphilis. 02:13 So you would want to rule those 2 things out. 02:16 Now in terms of treating the contacts of the patients – someone who’s had sex with a patient within 10 days before the onset of symptoms – they need to be identified and treated. 02:31 Even asymptomatic contacts of people you thought had chancroid should be treated, and the treatment is simple with 1 gram of azithromycin in a single dose. 02:45 Lastly let's have a view on fluctuant lymph nodes. They should be aspirated, or if they are very large or infected, an incision and drainage maybe needed.
About the Lecture
The lecture Chancroid: Diagnosis and Therapy by John Fisher, MD is from the course Genital and Sexually Transmitted Infections.
Included Quiz Questions
Which of the following tests confirms the diagnosis of chancroid in a patient with a typical clinical presentation?
- Polymerase chain reaction
- Gram stain
- Blood culture
- Serology
- A typical clinical presentation alone confirms the diagnosis.
What is the first-line treatment for chancroid in a patient without allergies?
- A single oral dose of azithromycin (1 g)
- Azithromycin 500mg twice a day for 7 days
- Clindamycin 900mg twice a day for 7 days
- Daily intravenous ceftriaxone (250 mg) for 10–14 days
- A single intramuscular dose of ciprofloxacin (250 mg)
A patient with a confirmed diagnosis of chancroid was treated with 1 gram of azithromycin as a single dose. He has not had any improvement despite 7 days of observation. Which of the following is the most appropriate next step in management?
- Ruling out coinfections including syphilis
- A Repeat dose of azithromycin
- A longer course of azithromycin (500mg twice a day for 7 days)
- A single dose of ceftriaxone (250mg)
- Treating sexual partners
Author of lecture Chancroid: Diagnosis and Therapy

John Fisher, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
