Playlist
Show Playlist
Hide Playlist
Cervicitis and Urethritis (Emergency Medicine)



-
Emergency Medicine Bord Sexually Transmitted Diseases.pdf
-
Download Lecture Overview
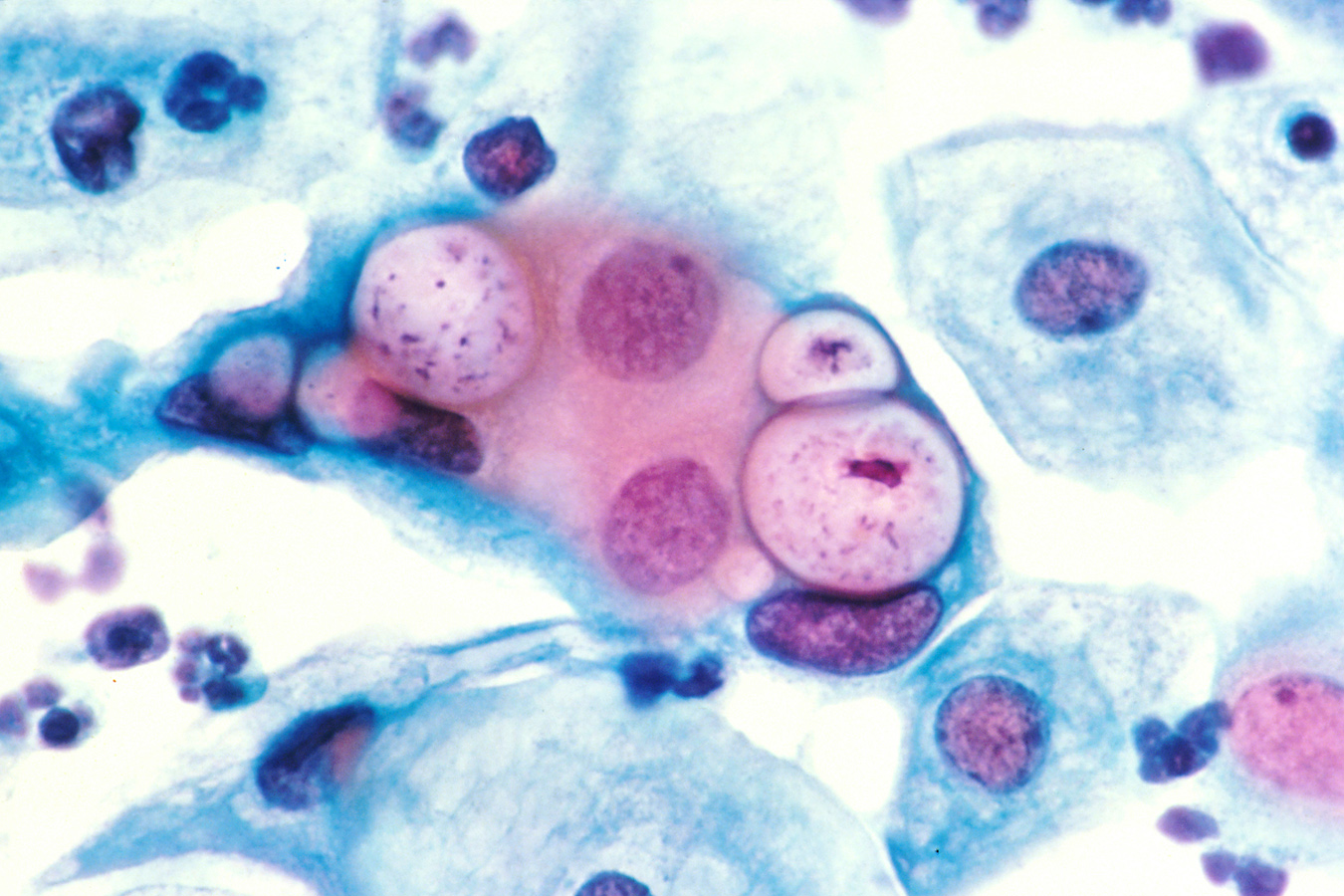
00:02 Hi. 00:02 We’re gonna be talking about genital urinary infections. 00:07 We’re gonna start out by talking about cervicitis and urethritis. 00:11 The most common organisms that cause these infections are gonorrhea, chlamydia and trichomoniasis. 00:20 When we’re talking about urethritis and cervicitis, we’re talking about a lower genital urinary tract infection. 00:26 So for the men that’s a urethral infection and for the women that’s an infection that goes to the level of the cervix. 00:34 What patients will be experiencing is they’ll be experiencing discharge. 00:38 This is characterized by the absence of lymphadenopathy and genital ulcers. So there won’t be any lesions that you’re gonna see on the patient’s genital area. 00:47 Patients may complain of dysuria, so burning when they urinate. 00:52 And then for female patients, they may have dyspareunia or post-coital vaginal bleeding. 00:58 Some patients of note maybe asymptomatic. 01:01 In these patients, one of the most important you can do is taking a sexual history. 01:05 So you wanna find out if your patient is sexually active. 01:08 If they use any barrier protection and also if they have sex with men, women, or both. 01:14 We’re gonna start out by talking about gonococcal urethritis. 01:17 Now, in the US there are over 300.000 cases of gonococcal urethritis annually. 01:23 The causative organism here is neisseria gonorrhea and humans are actually the only reservoir for this infection. 01:30 For male patients they have a lot of discharge. 01:32 So no GU lecture would be complete without a picture of some discharge from a GU infection. 01:39 And for female patients, they have high a rate of asymptomatic infection and this is concerning because although the cervicitis maybe asymptomatic. So the lower GU infection is not gonna cause them a lot of symptoms. 01:51 This can have a high rate of ascending infection. 01:54 So infection that would go to the uterus, the fallopian tubes, possibly even the ovaries. 01:59 So we wanna make sure that we’re thinking about this diagnosis and that we’re diagnosing it before it gets to the situation that it's an upper genital urinary tract infection. 02:09 Now, thinking about gonococcal urethritis, one of the big things to also consider is that gonococcus can also cause pharyngitis. 02:17 So patients can have an infection in their throat. 02:22 You can have a disseminated infection. Patients who have disseminated gonococcal infections can have fevers. 02:28 They can have a pustular rash potentially. 02:32 Septic arthritis. 02:33 This is a common cause or a more common cause of joint swelling and septic joint in a younger patient or a patient who’s engaged in risky behavior. 02:42 So patients who come in with a single joint that’s swelling. 02:44 Classically, gonorrhea will settle in the knee. 02:47 You wanna make sure you’re thinking about gonorrhea on the differential. 02:52 And then conjunctivitis as well. 02:53 So not only can it cause a urethritis, a cervicitis, an ascending GU infection. 02:58 It can also go ahead and cause lots of systemic processes and a systemic infection. 03:06 Now we’re gonna move on next and we’re gonna talk about chlamydia. 03:09 Chlamydia is the most commonly reported STD in the United States. 03:12 And chlamydia actually also has very high rates of asymptomatic infections. 03:18 Adolescents and young adults have the highest rate of infection. 03:22 And it’s important to note that chlamydia generally has less discharge associated with it than gonococcal urethritis. 03:30 If untreated though, this also can progress to an upper tract infection. 03:34 So can ascend into the uterus, the ovaries, the fallopian tubes in women and develop PID. 03:40 And in men it can develop into epididymitis or orchitis. 03:44 And I will be talking about those a little bit later in this lecture. 03:49 Now, how do we diagnose gonorrhea and chlamydia? One important thing to consider is that there's often times a co-infection. 03:56 So patients often times have both gonorrhea and chlamydia at the same time. 04:00 And it’s very difficult to distinguish between the two of these based on your exam, your history. 04:08 The testing that we send is a PCR test or a nucleic acid amplification test. 04:13 That test has a 90-100% sensitivity and a 99-100% specificity. 04:20 You can send the specimen from the cervix, from the vagina, from the urethra or also from a first void urine. 04:27 It’s important to note, do you wanna have a first void urine and if you’re gonna be sending the test from the urine that you don’t wanna have the patient use a cleansing wipe in that area because essentially that can wipe away some of the chlamydia or gonorrhea that’s present there. 04:43 You also wanna consider other labs depending on where the patient is complaining of symptoms. So potentially an oral pharyngeal swab or a rectal swab maybe indicated depending on the patient’s history. 04:56 Now, when we’re treating these patients, we generally will treat for both gonorrhea and chlamydia. 05:00 Because what happens is you send off that nucleic acid amplification test and those results actually take about 24-48 hours depending on your lab and how frequently they ran that test for those results to come back. 05:14 So what this involves, is it involves a conversation with your patient. 05:17 So if you’re concerned that someone has urethritis or cervicitis, you have to engage that patient in conversation and discussion. 05:26 I always explain to patients that the results for the test aren’t gonna be back for about 24-48 hours and we always have a discussion about whether or not they are very suspicious that they may have a genital infection or whether they’re not. 05:39 You can imagine that there’s a lot of social implication here. 05:42 If someone thinks or believes that they’re in a monogamous relationship and they haven't had intercourse with anyone outside of the relationship, but the potential implication is that their partner maybe having an unfaithful portion of the relationship, him or her. 05:58 So we definitely wanna make sure we’re having that discussion with patients, because it really can have a lot of implications for their lives and moving forward in their relationships. 06:10 And when we go ahead and treat the classic regimen is that we give azithromycin 1 gram orally or you can give doxycycline 100 milligrams PO twice a day for 7 days. 06:22 Now, for the most part, we give the azithromycin one gram orally in the Emergency Department. 06:27 Because what happens is you give the patient the medication, they take it, they’re done. 06:31 When someone goes home if they're prescribed doxycycline for 7 days, you can imagine that patient might not always be compliant with taking medication. 06:39 It can be hard to remember, they might not be able to fill their prescription for a few days. 06:44 So often times, as long as the patient can tolerate it, we go ahead and give azithromycin. 06:48 You know, that is a large dose actually of azithromycin and can sometimes be associated with nausea and vomiting after people get it. 06:56 So sometimes depending on the patient, a pre-treat term with a little bit of nausea medication or if they start to feel nauseous after they take it, we'll give them a little bit of anti-nausea medication in the ED. 07:08 The other medication that’s part of this regimen is ceftriaxone. 07:11 It’s administered intramuscularly, and the dose is 500 mg. 07:17 Patients aren’t often times very excited about having to get this shot and it can be a little bit painful. 07:23 Sometimes, nursing will mix it with a little bit of lidocaine to decrease the amount of pain associated with that injection.
About the Lecture
The lecture Cervicitis and Urethritis (Emergency Medicine) by Sharon Bord, MD is from the course Abdominal and Genitourinary Emergencies. It contains the following chapters:
- Cervicitis and Urethritis
- Cervicitis and Urethritis Diagnosis
Included Quiz Questions
What is the causative organism for gonococcal urethritis?
- Neisseria gonorrhea
- Neisseria meningitidis
- Chlamydia trachomatis
- Chlamydia psittaci
- Chlamydia pneumoniae
What is the most commonly reported sexually-transmitted disease in the United States?
- Chlamydia
- Herpes
- Gonorrhea
- Chancroid
- Genital warts
What is the highly specific and highly sensitive test used to diagnose gonorrhea and chlamydia?
- Nuclei acid amplification test
- Pap smear
- Urinalysis
- FTA-ABS
- VDRL test
What first-line drug is preferred for the treatment of cervicitis and urethritis, given as a single dose in combination with ceftriaxone?
- Azithromycin 1 g
- Azithromycin 500 mg
- Ciprofloxacin 500 mg
- Metronidazole 500 mg
- Cefuroxime 1 g
Author of lecture Cervicitis and Urethritis (Emergency Medicine)

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
