Playlist
Show Playlist
Hide Playlist
Celiac Disease (Sprue): Definition and Treatment

-
Slides Small and large bowel.pdf
-
Download Lecture Overview
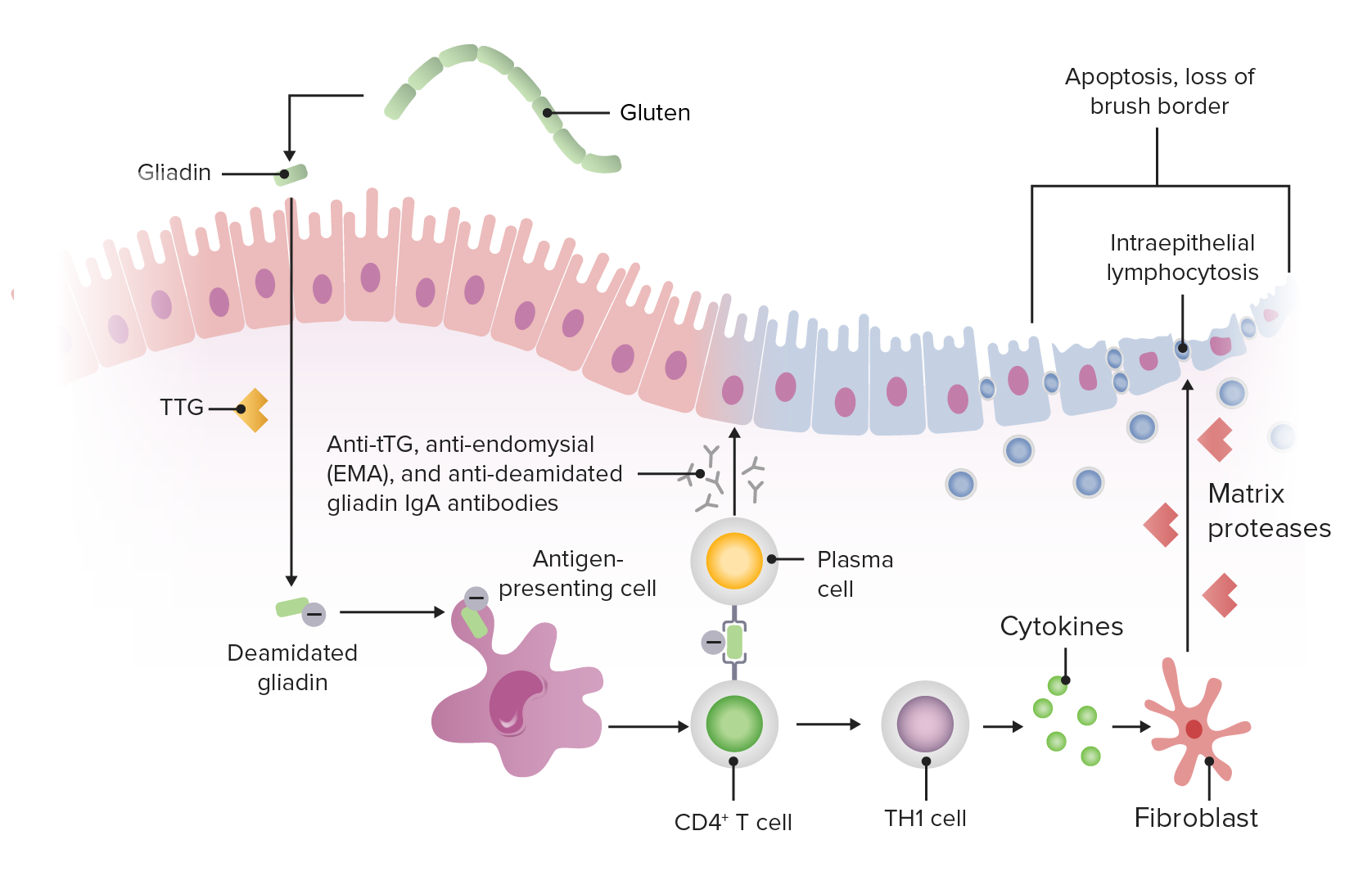
00:01 Our topic now brings us to Celiac Sprue. 00:03 Now, Celiac Sprue is extremely marketable in terms of the products that we find everywhere in the US. 00:12 You´re going to the grocery store, gluten-free diet or gluten-free products. 00:16 You walk into a pizzaria, there´s gluten-free crusts. 00:20 So, obviously here we have an issue where the body is then creating an autoimmune type of status in which now, anywhere along the GI tract, you might have destruction taking place. 00:35 Welcome to Celiac disease. 00:37 In the US the prevalence is as high as 1 in 200. 00:42 Diarrhea is not the main symptom in adult. Doesn´t have to be. 00:45 Iron deficiency is much more common. 00:49 Remember that Celiac Sprue, you should be thinking about being in the intestine where the lesion is taking place and it can pick and choose us to whatever it wants in terms of what it wants to destroy. 01:01 It doesn´t have to be continuous. Maybe it´s destroying the duodenum. 01:05 Maybe it might skip over down to the jejunum or maybe perhaps even down to terminal ileum resulting in B12 deficiency. 01:12 So malabsorption is a big issue in Celiac. 01:16 Once you start destroying the parts of the intestine everywhere, at some point in time, there is some kind of malabsorption for sure taking place maybe perhaps even vitamin D and therefore resulting to osteomalacia in your patient. 01:30 Associated with, apart from the intestine and diarrhea that might be associated in malabsorption on the skin there´s an extra intestinal manifestation, it looks like herpes but it´s not. 01:43 We call this dermatitis herpetiformis which you would expect upon biopsy here would be immunoglobulin A and only reason for that is because, remember, the type of immunoglobulin that you have in your GI system is IgA. 01:58 The increased incidence of small bowel lymphomas and juvenile diabetes mellitus. 02:05 Other autoimmune conditions could also be associated with Celiac Sprue. 02:10 Here is the skin manifestation that looks like herpes but it´s not. 02:16 This is a patient that is suffering from Celiac disease. 02:19 Now, we go ahead and call this dermatitis herpetiformis. 02:23 Do not forget this and do not choose anything. 02:26 Make sure that you pay attention to the proper histories. 02:28 So if there´s a history in the patient of may be consuming wheat and bread and such and apart from having malabsorption syndrome, have issues in the skin, this is Celiac. 02:39 Diagnosis: We´re looking for what´s known as tissue transglutaminase, anti-endomysial, anti-gliadin antibodies. I would know all three. 02:53 You need to know all three. Transglutaminase, anti-endomysial and gliadin antibodies for diagnosis. What then happens to the intestine? Remember, if by chance it´s the duodenum that´s being affected which normally should have all of that finger-like villi, it gets blunted and when it becomes blunted, then you worry about malabsorption. 03:18 How do you manage a patient with Celiac? Well, if you know that the patient is most likely having exacerbations after consumption of these food products that contain gluten. 03:30 Well, obviously gluten-free diet becomes highly recommended. 03:34 Relapses usually either dietary non-compliance or cross-contamination and as we mention earlier whenever you have an autoimmune disease, and I mean anywhere in the body including Hashimoto, including autoimmune disease with pernicious anemia or autoimmune disease such as celiac, lymphomas is something that you´re paying attention to. 03:59 Corticosteroids for refractory cases. 04:04 What you´re seeing here in fact with Celiac is the fact that in the duodenum, there is absolutely no microvilli. It´s being completely blunted. 04:16 On top where we are here is the intestine and the lumen would be on the top portion of this picture and normally should have little finger-like villi that is responsible for reabsorption increasing surface area. That has been lost in Celiac.
About the Lecture
The lecture Celiac Disease (Sprue): Definition and Treatment by Carlo Raj, MD is from the course Small and Large Intestine Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following tumors is associated with celiac sprue?
- Small bowel lymphoma
- Small bowel adenocarcinoma
- Small bowel GIST
- Small bowel polyp
- Small bowel carcinoid
Which of the following diseases is NOT associated with malabsorption due to celiac sprue?
- Hashimoto's thyroiditis
- Dermatitis herpetiformis
- Iron-deficiency anemia
- Osteomalacia
- Pernicious anemia
Which of the following antibodies are associated with celiac sprue?
- Anti-endomysial antibodies
- Anti-ssb antibodies
- Anti-Ro antibodies
- Anti-dsDNA antibodies
- Anti-centromere antibodies
What is the microscopic finding seen in celiac sprue?
- Complete flattening of villi with intraepithelial lymphocytes
- No flattening of villi with intraepithelial lymphocytes
- Transmural inflammation with crypt abscess
- Mucosal inflammation with lymphocyte aggregates
- Sloughing of mucosa with many neutrophils
Which immunoglobulin can be isolated by a biopsy of the dermatitis herpetiformis lesion associated with celiac sprue?
- IgA
- IgM
- IgG
- IgE
- IgD
Author of lecture Celiac Disease (Sprue): Definition and Treatment

Carlo Raj, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
clarified some of my misconceptions like the type of nutritional def associated with the condition and which parts of the bowel is affected. I am unsure why people gave it 3 star.
A superficial talk about an important contributor to malabsorption. I think it would have been good to discuss why we need to assess for the prescence of IgA to begin with. What the role of HLA is in the disease. Moreover, the importance of biopsy as well as the long term complication of celiac disease include osteoprosis, neurological impairment and enteropathy associated T-cell lymphoma.
