Playlist
Show Playlist
Hide Playlist
Case: 68-year-old Man with Progressive Altered Mental Status and Gaze

-
Slides Head Trauma Subdural Hemorrhage.pdf
-
Download Lecture Overview
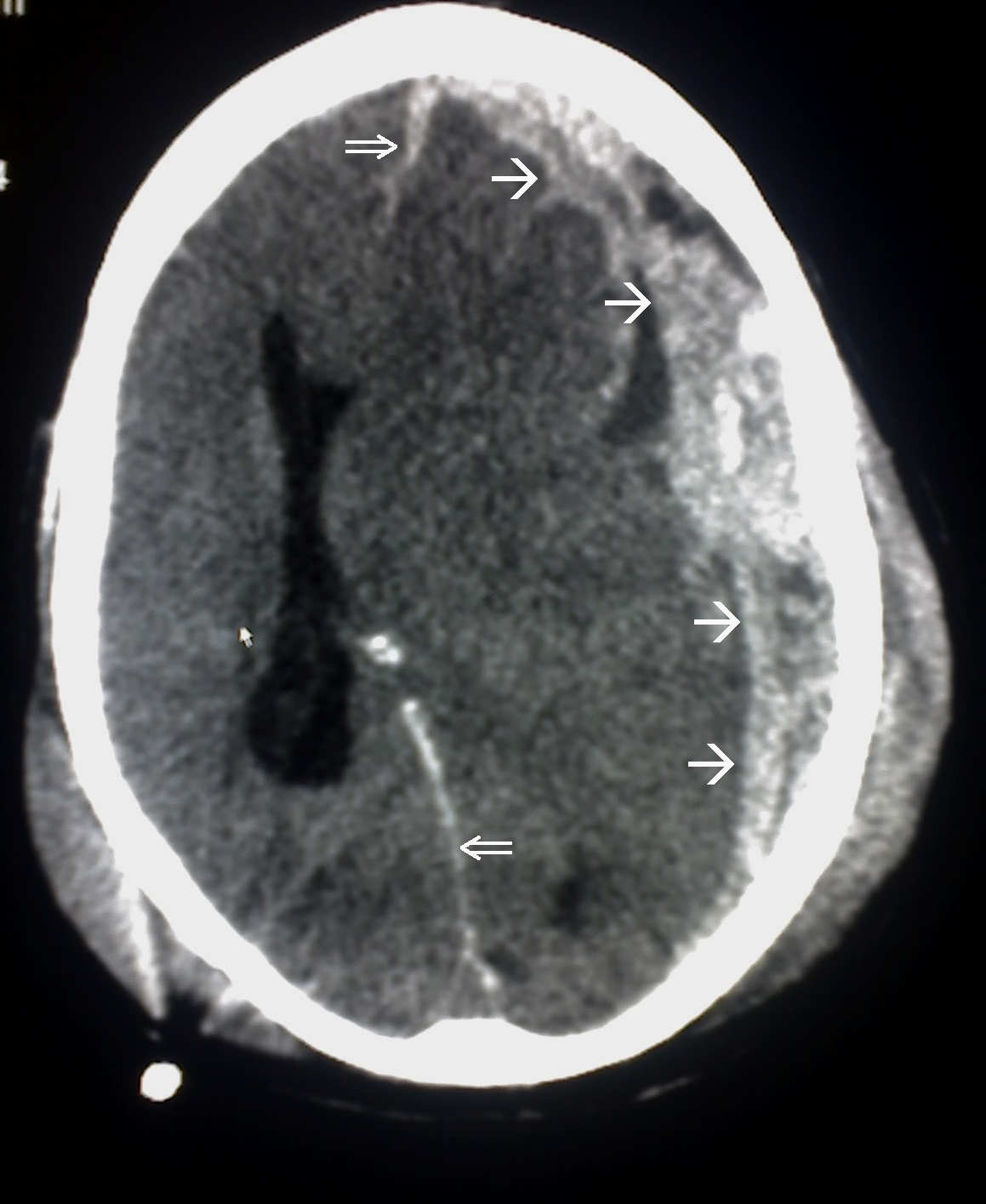
00:02 In this talk, let's review subdural hematomas. 00:07 So let's go back to our case. 00:09 This is our 68 year-old man with no significant past medical history who presents to the emergency department with progressive altered mental status. 00:16 The patient initially fell from a small ladder at his home 4 days ago. 00:20 His family says that he appeared normal immediately after the fall. 00:23 Over the past few days, he's become progressively weaker and began to trip on his right leg and have reduced use of his right arm. 00:31 Today, the patient began to become progressively more confused and has not been speaking. 00:36 On examination, he is awake. 00:38 His eyes are open spontaneously. 00:40 He has a left gaze preference but is able to look past midline. 00:43 He moves to the left side of his hemibody with full strength, but has significant right hemiparesis and is only able to withdraw with pain. 00:53 He undergoes imaging non-contrast head CT, demonstrating a crescent-shaped hyper density over the left cerebral convexity with associated midline shift. 01:05 After initial admission, and close monitoring the patient's exam improves initially. 01:10 And then over the following 24 hours, he progressively declines. 01:15 A repeat head CT is performed. 01:18 And we see that here. 01:19 Now we see a mixed area of blood with some hyperdense blood posteriorly and more isodense blood over the left convexity. 01:29 We see the thickness of the blood has increased. 01:32 There's more significant midline shift and underlying mass effect on the brain. 01:36 And this is likely contributed to this patient's clinical decline. 01:41 So what's the best next step in managing this patient? Should we start levetiracetam for presumed seizure as the cause of his decline? Should we initiate reversal agents for coagulopathy consult neurosurgery for evacuation, or burr hole drainage or perform an MRI to really characterize this hemorrhage and any underlying brain injury? Well, starting levetiracetam for presumed seizure is not necessarily a problem in patients where we suspect seizure, but this patient's decline is not indicative of seizure. 02:13 He's had hematoma expansion which is more likely to contribute to his neurologic decline. 02:19 Initiating reversal agents for a coagulopathy as needed if there is a coagulopathy. 02:24 But there's no suggestion based on this patient's past history or current events of underlying coagulopathy as the cause for hematoma expansion. 02:33 MRI can be performed and would help us to evaluate underlying brain injury. 02:37 But the CT is sufficient for understanding what's going on with this patient. 02:41 And that is expansion of hematoma. 02:43 And this requires management as opposed to evaluation. 02:47 And so here the right answer is to consult neurosurgery either for evacuation or burr hole drainage. 02:53 And in this patient, neurosurgery did perform an evacuation of this blood and we can see the post operative imaging. 02:59 We see reduction in the size of the hemorrhages there's still a little bit of hemorrhage along the left convexity. 03:04 The mass effect and midline shift had been resolved in this patient's clinical exam dramatically and rapidly improved as a result of surgery.
About the Lecture
The lecture Case: 68-year-old Man with Progressive Altered Mental Status and Gaze by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
What diagnosis is suggested by the finding of a crescent-shaped opacity on non-contrast CT head imaging?
- Subdural hematoma
- Epidural hematoma
- Subarachnoid hemorrhage
- Intraparenchymal hemorrhage
- Amyloidosis
What is the next best step in management for a patient with a subdural hematoma, significant midline shift, and declining mental status?
- Neurosurgical consultation
- Seizure prophylaxis
- MRI
- PET scan
- Reversal of coagulopathy
Author of lecture Case: 68-year-old Man with Progressive Altered Mental Status and Gaze

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
